Wael A. Alqarawi, MD, Kamran M. Khan, MD, MPH, Arlene S. Bierman, MD, MS
Wael A. Alqarawi, MD, is from the Internal Medicine Program, University of Toronto, Ontario, Canada. Kamran M. Khan, MD, MPH, is from the Department of Medicine, Division of Infectious Diseases, Li Ka Shing Knowledge Institute of St. Michael’s Hospital, Toronto, Ontario, Canada. Arlene S. Bierman, MD, MS, is from Lawrence S. Bloomberg Faculty of Nursing, University of Toronto, Ontario, Canada, and the Department of Medicine, Department of Health Policy, Management and Evaluation, Public Health Sciences, Li Ka Shing Knowledge Institute of St. Michael’s Hospital, Toronto, Ontario, Canada.
The authors reported no potential conflict of interest relevant to this article.
Consider referral to an infectious disease specialist for patients coinfected with HTLV-1, as well as those who are immunocompromised. Such referral also may be appropriate for patients from countries where loa loa is endemic, because encephalopathy has occurred in patients coinfected with loa loa who were treated with ivermectin.10
Our patient was treated with 2 doses of ivermectin 200 mcg/kg, 2 weeks apart. Four months later, his eosinophilia had resolved, his IgG-ELISA dropped to 0.37, and he had gained 2.5 pounds.
THE TAKEAWAY
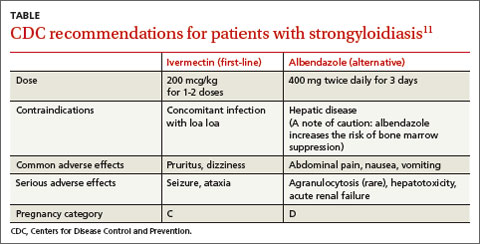
Strongyloidiasis is an infection caused by the parasitic worm Strongyloides stercoralis that is most common in tropical or subtropical areas. It can be asymptomatic or present with a wide range of nonspecific signs and symptoms, such as eosinophilia, cough, wheeze, abdominal pain, weight loss, diarrhea, pruritus ani, and larva currens. It is diagnosed by stool examination and serologic testing. Ivermectin is first-line therapy; albendazole is an alternative.