Case c. This patient was punctured by a sago palm thorn, but believes that she removed the entire thorn at the time of injury. A small puncture wound is seen on physical exam, and x-rays are unremarkable. The patient is placed on a 10-day course of oral cephalexin. At follow-up, she has swelling in an adjacent finger.
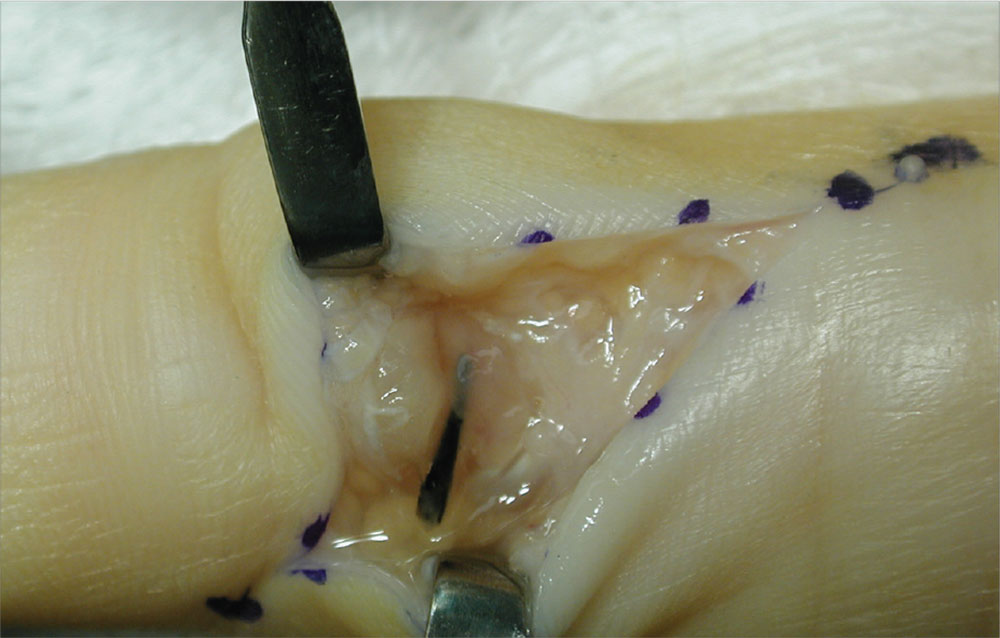
The palmar puncture wound site was surgically explored, and no foreign body fragments were found. In addition, the tendons, retracted and delivered through the skin incision, appeared normal.
Histopathology of a specimen intraoperatively biopsied from the flexor tendon sheath showed some refractile foreign material consistent with plant material. After surgery, swelling persisted, and the patient developed limited motion at the extremes of active flexion and extension.
After 2 months, the decision was made to re-explore the palmar puncture site and flexor tendon and obtain tissue specimens for culture, including atypical mycobacterial and fungal cultures. During the second surgery, the palmar site and flexor tendon still appeared unremarkable. As there was some swelling in the long finger, the flexor tendon sheath was explored distally through a separate incision over the middle phalanx. A transversely oriented fragment of the sago palm thorn was found within the flexor tendon sheath. Flexor tendon sheath material was cultured and subsequently found to be negative.
For more information, see “Distal Migration of a Foreign Body (Sago Palm Thorn Fragment) Within the Long-Finger Flexor Tendon Sheath.” Am J Orthop. 2008;37(4):208-209.