in this population, according to the authors of a clinical review article on the topic.

Dr. Andrew Alexis
“Current reports of rosacea in patients with skin of color may point to a large pool of undiagnosed patients,” said Andrew F. Alexis, MD, chairman of the department of dermatology, Mount Sinai St. Luke’s and Mount Sinai West, New York, and his coauthors.
Increased awareness of rosacea in these patients may reduce disparities in disease management, they wrote in the review, published in the Journal of the American Academy of Dermatology, which outlines strategies for timely diagnosis and effective treatment of rosacea in skin of color.
The erroneous perception that rosacea does not occur in skin of color may arise from epidemiologic reports, which frequently position it as a disease that occurs in fair-skinned individuals of Northern European or Celtic background, they said.
The reported prevalence of rosacea in skin of color varies worldwide and is as high as 10%, according to the authors. Moreover, a recent U.S. medical care survey found that 3.9% of rosacea patients were Hispanic or Latino, 2.3% were Asian or Pacific Islander, and 2% were black.
 Jerry Tan, MD, University of Western Ontario/National Rosacea Society
Jerry Tan, MD, University of Western Ontario/National Rosacea Society
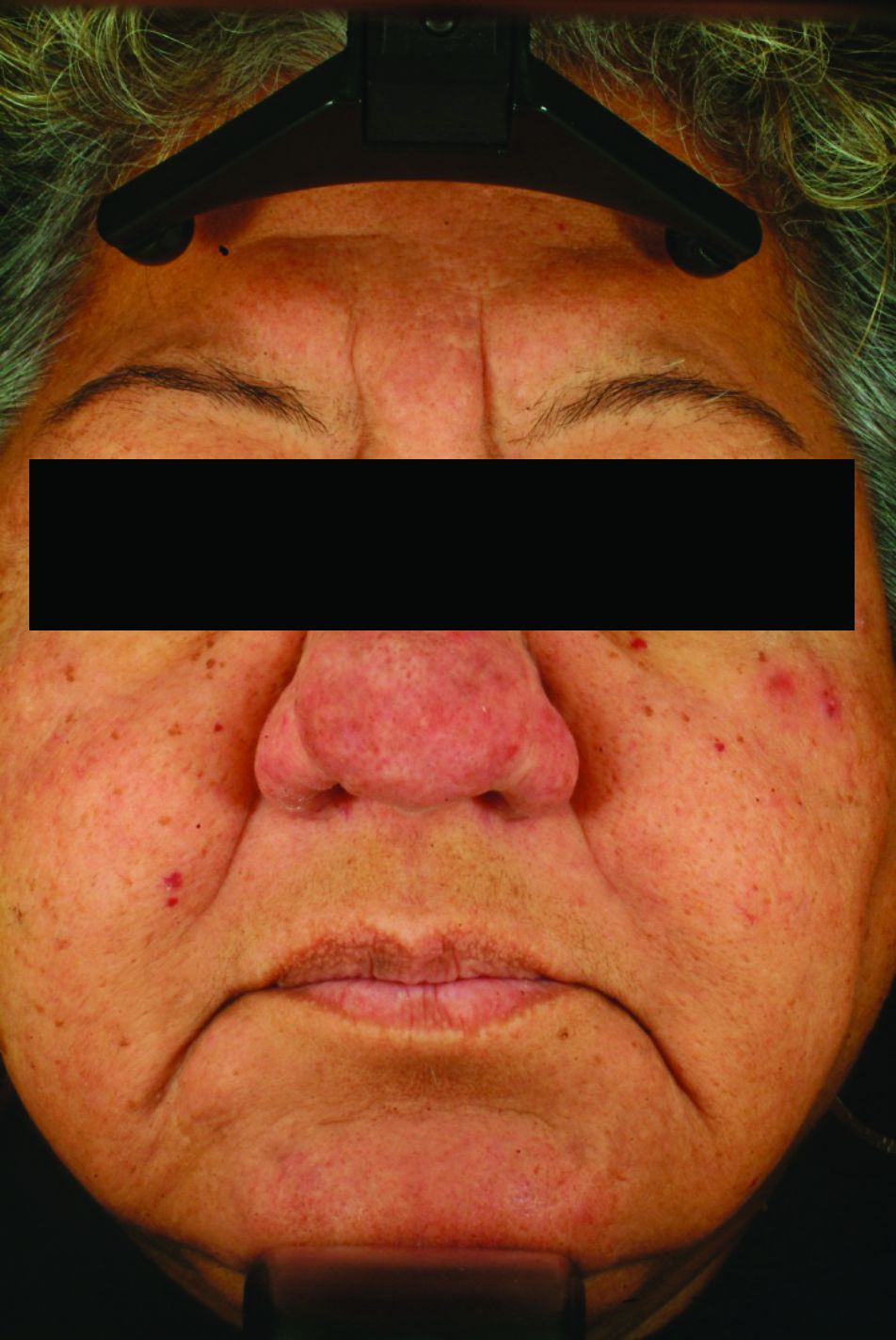
Rosacea: A Latina woman with inflammatory rhinophyma
A low index of suspicion for rosacea in skin of color may lead to delayed diagnosis, and consequently, advanced disease that could include disfigurement with disease progression (such as rhinophyma and otophyma) and, in the case of ocular disease, loss of sight, Dr. Alexis and his coauthors pointed out.
One clinical aspect of rosacea in skin of color is that persistent facial erythema is less frequently reported than are papules and pustules. That may be due to the difficulty of visualizing erythema in darker skin, they suggested, noting that the postinflammatory hyperpigmentation that is more common in skin of color could also mask erythema.
A rosacea variant seen more often in these patients is the granulomatous subtype, which may not present with flushing, persistent erythema, or other typical rosacea signs, they pointed out.
 Jerry Tan, MD, University of Western Ontario/National Rosacea Society
Jerry Tan, MD, University of Western Ontario/National Rosacea Society
Rosacea: Latina woman with inflammatory rhinophyma
One key to accurately diagnosing rosacea in skin of color is the patient’s own observations, such as whether they experience flushing or a warm sensation in the face, according to the authors, who said patients may report stinging or burning with certain skin care products.
Dr. Alexis and his coauthors said they have tried various strategies to assess dark skin for erythema and telangiectasia. Photographing subjects on a dark-blue background may better highlight any redness, they said, while using a dermatoscope may help differentiate skin pigment from blood vessels.
A magnifying glass or microscope slide can be used to test skin for blanching: “If the skin pales when pressed under the glass or slide, erythema is present,” they wrote.
 Ncoza Dlova, MD, chief specialist and head of the department of dermatology, Nelson R. Mandela School of Medicine, Durban, South Africa/National Rosacea Society
Ncoza Dlova, MD, chief specialist and head of the department of dermatology, Nelson R. Mandela School of Medicine, Durban, South Africa/National Rosacea Society
Rosacea with phymatous changes in an African woman
Although data on treatment of rosacea in skin of color is limited, the general treatment approach is similar to that of lighter skin and may include topical and oral therapies, laser or light-based treatment, or surgery. “Patients with skin of color may have unique clinical features that need to be addressed during the treatment of rosacea, such as postinflammatory pigment alteration or risk of developing this complication with laser/light-based therapies,” they noted.
In the review, they referred to a few studies of oral or topical treatments that suggest similar benefits in Fitzpatrick skin phototypes I-III (lighter) and IV-VI (darker) that the authors describe in their review.
Allergan sponsored development of the paper, which was developed with editorial assistance from Peloton Advantage. Dr. Alexis and his coauthors provided disclosures related to Allergan, BioPharmx, Galderma, Bayer, Beiersdorf, Croma-Pharma, Aclaris, and Unilever.
SOURCE: Alexis AF et al. J Am Acad Dermatol. 2018 Sep 18. pii: S0190-9622(18)32576-3. doi: 10.1016/j.jaad.2018.08.049.