The Adams forward bend test should be conducted.24,25 The child who is able to stand faces away from the examiner, then bends forward at the waist with the knees straight and the arms hanging down passively (see Figure 2). The practitioner looks at the spine from behind and notes any rib, thoracic, scapular, or lumbar prominence that could indicate a rotational spine deformity.1,4,7 In some instances, the use of a scoliometer can be helpful to assign a number to the amount of rotation to the spine during the Adams forward bend test. However, primary care offices are not often equipped with this device.26
Motor and Neurologic Examinations
The motor exam includes testing motor strength in all four extremities and noting any asymmetry. The examiner should have the child actively bend in every direction, making note of any deformity, stiffness, or asymmetry. The patient's spine should be palpated, with any tenderness noted, and any available radiographs reviewed.1,4,7
The neurologic exam includes testing cranial nerves, sensation, and reflexes, including the patellar, Achilles, and umbilical reflexes, as well as Babinski's sign. Many patients are areflexic in one or more areas. For instance, a finding of no umbilical (abdominal wink) reflex on either side is not suspicious in itself, but it should alert the practitioner to evaluate carefully for asymmetrical reflexes in one or more areas, especially if they are ipsilateral. Any positive neurologic findings, especially in the setting of scoliosis, warrant an MRI.1,7
Scoliosis Screening in the School Setting
One controversial subject related to scoliosis is school screenings. These screenings were developed in the 1980s for early identification of children with scoliosis curves so that nonsurgical treatment could be initiated promptly, or that surgery, when deemed necessary, could be performed in a timely fashion for optimal results.27
Since then, the effectiveness of screening programs has come under debate; in 2004, the US Preventive Services Task Force28 issued a recommendation (rating, "D Recommendation") against routine screening for idiopathic scoliosis in asymptomatic adolescents, stating that its effectiveness had not been shown in clinical trials. In response, a task force was convened by the American Academy of Orthopaedic Surgeons, the Scoliosis Research Society, the Pediatric Orthopaedic Society of North America, and the American Academy of Pediatrics, with findings published in a 2008 information statement by Richards and Vitale.25 While acknowledging the limitations of support for screening in the literature, the task force concluded:
- Early treatment of the deformities associated with idiopathic scoliosis can result in substantial benefits
- Screening (whether in the school environment or other settings) offers an opportunity for early diagnosis and appropriate referral of otherwise undetected deformities, especially in under-served populations
- In many cases, brace treatment may preclude the need for surgery in children with significant scoliosis
- Identifying deformities that require surgery as early as possible through screening increases the likelihood of good treatment outcomes
- Girls, who reach adolescence two years earlier than boys, should be screened at ages 10 and 12; boys, at age 13 or 14
- School personnel who conduct screening should receive training to detect spinal deformities
- While no screening test is entirely reliable, the forward bend test is considered the most specific test for detection of scoliosis29
- The participating organizations remain committed to preventing inappropriate use of spinal x-rays.25
Despite the ongoing debate, more than half of the US states have screening programs in place.24,27
RADIOGRAPHS/LABORATORY TESTING
Physical examination and a thorough history are most important in evaluation for scoliosis in the primary care setting. When radiographs (x-rays) are considered necessary, posterior-anterior and lateral spine series should be ordered. These are full-length (3-ft)
x-rays of the patient standing with the knees straight (when the child is able to do so).1,4,7 The x-rays are taken in the posterior-anterior direction to minimize breast and organ radiation exposure and to produce an x-ray similar to that of viewing the patient from behind.
If scoliosis is observed on radiography, note the apex of the curve, the location, the direction in which it curves, and any rotational component. Examine for pelvic obliquity, shoulder asymmetry, spondylosis, or spondylolisthesis.7
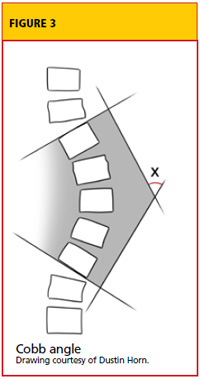
The Cobb angle is the measurement used to quantify the degree of scoliosis.4,5,7 Using the posterior-anterior radiograph, a line is drawn along the superior endplate of the most curved cephalad vertebra and the inferior endplate of the caudal vertebra. When perpendicular lines are drawn, the intersecting lines form the Cobb angle (see Figure 3, in which "X" indicates the Cobb angle, measured in degrees). An increasing angle reflects the increasing severity of scoliosis.
Other radiographs that may be ordered include supine lateral (bending) x-rays or supine traction radiographs to evaluate curve flexibility before surgery30; recently, hanging total spine x-rays have been investigated to evaluate spine flexibility before brace treatment.31 Additionally, hand/wrist x-rays may be ordered to determine the patient's remaining growth potential. These are most often taken in an orthopedist's office.3