DIFFERENTIAL DIAGNOSIS
Not all patients with symptoms suggestive of IM are found to be infected with EBV. Other pathogens may be responsible for primary infection in these patients10 (see Table 15,10,12,17-20).
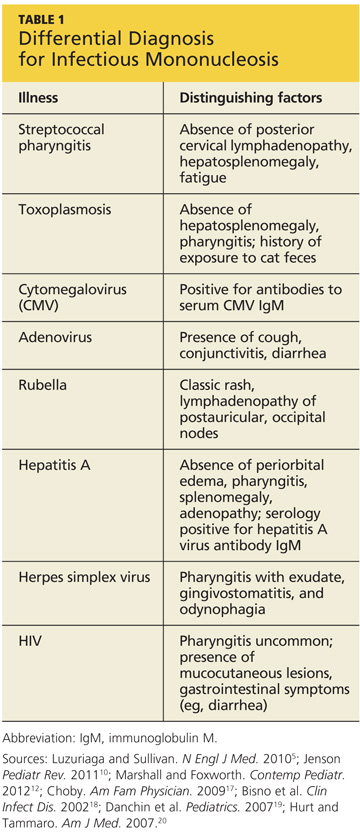
Streptococcal pharyngitis is the illness most likely to be confused with IM because of the similarity of symptoms; one in four children with acute sore throat (as well as 5% to 20% of affected adults) may be infected with group A beta-hemolytic streptococcus (GABHS).17-19 Although, in addition to sore throat, patients with GABHS may experience localized swelling of the anterior cervical lymph nodes, GABHS is not usually characterized by posterior cervical lymphadenopathy. Additionally, the hepatosplenomegaly and fatigue common to IM would not be present in patients with streptococcal pharyngitis.5
GABHS is confirmed by a positive throat culture for group A streptococcus17; in patients with negative results on a rapid antigen test, IM should be considered in the differential diagnosis.
Toxoplasmosis can manifest with symptoms similar to those of EBV-associated IM. The classic IM symptoms of hepatosplenomegaly and pharyngitis are not often seen in cases of toxoplasmosis, however. The history should reveal contact with cat droppings or cat litter.12,20
Patients infected with cytomegalovirus (CMV) can present asymptomatically or with the common triad of symptoms of IM. Splenomegaly, malaise, and lymphadenopathy may be present. A diagnosis of CMV is confirmed by the presence of antibodies to serum CMV IgM.12,20
Adenovirus typically manifests with cold-like symptoms, cough, conjunctivitis, and diarrhea. The triad of symptoms typically seen with IM may be present with decreased severity in patients with adenovirus. Culture of nasopharyngeal swabbings can confirm a diagnosis of adenovirus.12,20
Symptoms of rubella can mimic those of IM, but the classic rubella rash should be a distinguishing factor. Lymphadenopathy most commonly affects the postauricular and occipital nodes. Parents may acknowledge that the patient has not been immunized against rubella.12
Manifestations of hepatitis A include hepatomegaly, fever, jaundice, abdominal pain, and fatigue. Symptoms associated with IM, including periorbital edema, pharyngitis, splenomegaly, and adenopathy, are not typically seen in patients with hepatitis A. Laboratory findings in the patient with hepatitis would include elevations in alanine aminotransferase and aspartate aminotransferase. Serology would be positive for hepatitis A virus antibody IgM and negative for EBV heterophile antibodies.12,16
Herpes simplex virus, commonly known as a cold sore, manifests with pharyngitis with exudate, gingivostomatitis, and odynophagia (painful swallowing). The appropriate polymerase chain reaction (PCR) test can be used to confirm the presence of herpes virus.12,20
HIV screening should be conducted in at-risk patients, as IM and HIV can present with similar symptoms of fever, malaise, lymphadenopathy, and rashes, especially in the early phase of primary HIV infection. Pharyngitis is less common in patients with HIV infection than in those affected by IM; rather, mucocutaneous lesions and gastrointestinal symptoms, such as diarrhea, are likely to be present.5 Diagnostic findings include a positive ELISA HIV antibody test and positive plasma viral load.12,20
On the next page: Diagnosis >>