DIAGNOSIS: OVERVIEW
VM is a diagnosis of exclusion that is considered appropriate when no other peripheral or central vestibular disorder is present to account for the patient’s dizziness.5,6 Asking the patient the right questions will provide clues to the correct diagnosis.7 Most patients with VM present with normal physical, vestibular, and neurologic examinations, especially if examined when symptom-free.5 In contrast, examinations for competing diagnoses often reveal abnormal findings.
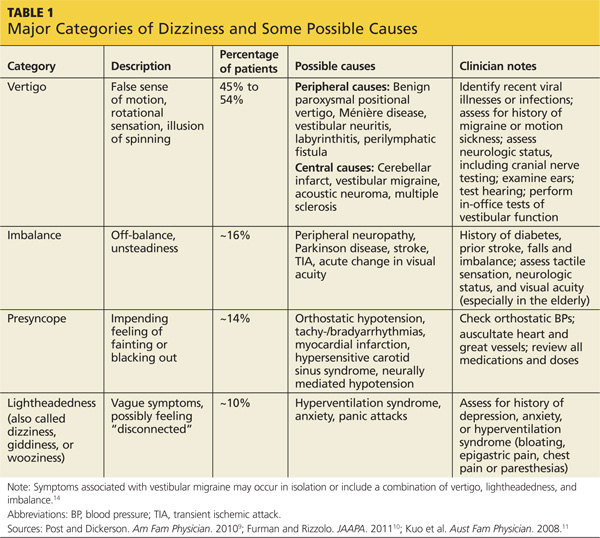
Vestibular vs nonvestibular vertigo. Typically, patients have difficulty describing their sensations with words more specific than “dizzy.”8 This lack of clarity is a challenge when the clinician is attempting to differentiate between true vertigo (ie, vertigo caused by vestibular dysfunction) and other types of nonvestibular dizziness. Specific categories of dizziness include vertigo, imbalance, presyncope, and lightheadedness; careful consideration must be given to the causes associated with each (see Table 1).9-11
Clinicians should focus on timing, duration of symptoms, triggers, and any other associated symptoms to determine the diagnosis.8,10 When evaluating a patient, a broad definition of vertigo, including spinning and/or rotational sensations as well as illusions of movement, is recommended.8
Peripheral vs central disorders. True vertigo must be further evaluated to determine whether its etiology is peripheral or central. In VM, a combination of both peripheral and central deficits can be seen.10 Clinicians must consider certain defining features to differentiate between these.
Peripheral Vertigo
If the cause of the patient's vertigo is peripheral, onset is often abrupt and the patient may experience mild-to-moderate imbalance that does not affect his or her ability to walk unassisted. Combined horizontal and rotational nystagmus may occur, which lessens or disappears with focused gaze. The nystagmus does not change direction when the patient gazes to either side and may fade after a few days.
The patient also may report experiencing tinnitus or hearing loss, accompanied by severe nausea or vomiting. Neurologic symptoms are rare in peripherally caused vertigo unless a concurrent diagnosis of migraine is confirmed.
Other symptoms may include weakness, dysarthria, changes in vision or hearing, paresthesias, changes in sensory or motor function, altered level of consciousness, and headache.10
Central Vertigo
Centrally caused vertigo often persists for hours to weeks, and neurologic symptoms are common. Patients have difficulty walking or standing still; problems with balance are severe. The nystagmus is purely horizontal, vertical, or rotational and may last for weeks to months. It is not inhibited with a focused gaze and may change direction with gaze. It is important to note that vertical nystagmus is 80% sensitive for vestibular nuclear or cerebellar central lesions.10
Tinnitus, if it occurs at all, is episodic, and nausea and/or vomiting vary from patient to patient. Patients presenting with central nervous system (CNS) disorders rarely complain of vertigo as their only symptom. Additional descriptions of dizziness may be used to describe the various cranial nerve abnormalities that suggest CNS etiology.9
DIFFERENTIAL DIAGNOSIS
Numerous conditions should be included in the differential when evaluating dizziness and vertigo symptoms. (See also Collie M. Vertigo: diagnosis and management. Clinician Reviews. 2013;23[12]:46-53.)
Peripheral Vertigo
Possible peripheral causes of vertigo include5,6,12,13
• Benign paroxysmal positional vertigo (BPPV)
• Vestibular neuritis
• Labyrinthitis
• Ménière disease
• Superior canal dehiscence
• Perilymphatic fistula
• Otitis media
• Aminoglycoside toxicity
• Trauma
BPPV is characterized by recurrent episodes of intense vertigo that last for seconds to one minute and are provoked by specific head movements. The Dix-Hallpike maneuver provokes vertigo and nystagmus and confirms the diagnosis.14 Vestibular neuritis and labyrinthitis present in similar ways. They are characterized by the onset of intense vertigo that can persist for several days, with nausea, vomiting, and imbalance also present. The main differentiating feature between them is associated hearing loss; vestibular neuritis is not associated with hearing loss, but labyrinthitis is. Both disorders are thought to be caused by inflammation of the vestibular nerve as the result of a viral infection. Patients may report recent upper respiratory infections or influenza like illnesses.10,12
Central Vertigo
Possible central causes of vertigo include5,6,13,15
• Acoustic neuroma (vestibular schwannoma)
• Cerebellar infarction
• Brainstem stroke
• Multiple sclerosis
• Episodic ataxia
• Psychogenic dizziness
Acoustic neuroma (vestibular schwannoma) is a benign growth on the vestibular nerve. Symptoms generally include progressive hearing loss and unilateral tinnitus accompanied by dizziness and imbalance.10 Acute attacks of vertigo are rare, but patients often complain of aural fullness, headache, and/or facial numbness.1,10
Cerebellar infarction usually presents with sudden onset of symptoms at maximal intensity. Risk factors for cerebellar infarction include a history of hypertension, coronary artery disease, diabetes, previous transient ischemic attack, smoking, alcohol consumption, atrial fibrillation, and hyperlipidemia.10
While only 5% of vertigo complaints are the result of CNS disorders, vertigo is an early symptom of brainstem stroke.15 Because of the significant morbidity and mortality associated with stroke, it must be considered in the initial diagnostic workup of vertigo.
Multiple sclerosis (MS) is an autoimmune disease in which the myelin axons in the CNS are destroyed. Dizziness and vertigo are common complaints associated with MS, but these patients will often present with other symptoms suggestive of CNS involvement. Common complaints include, but are not limited to, muscle weakness, fatigue, paresthesias, spasms, ataxia, pain, diplopia, dysarthria, heat intolerance, and urinary frequency.16
Episodic ataxia type 2 (EA2) is an inherited autosomal dominant disorder characterized by attacks of ataxia, vertigo, and nausea that can last from minutes to days. EA2 is often difficult to differentiate from VM due to symptom overlap. Fifty percent of patients with EA2 have a history of migraine headaches; often, there is a family history of similar symptoms.5
On the next page: Ménière Disease Versus VM >>