Prior to placement, patients must have had a failed course of conservative pain management and have no surgical options, no medical contraindications (eg, spinal pathology or susceptibility to infection), and no evidence of active addiction.12 A medication history is crucial, too, to identify use of anticoagulation therapy—a relative contraindication—as well as drug allergies and potential drug-drug interactions to guard against.3
An IT trial may be required
It is common practice for patients to undergo an IT analgesia trial prior to implantation of a subcutaneous pump. This involves using an external pump to infuse the selected medication intrathecally and slowly titrating it according to symptoms for 2 to 3 days. During this time frame, the patient records his or her response; a reduction by more than half in VAS pain score is considered a success, indicating that the patient is an appropriate candidate for placement of the device.3,13
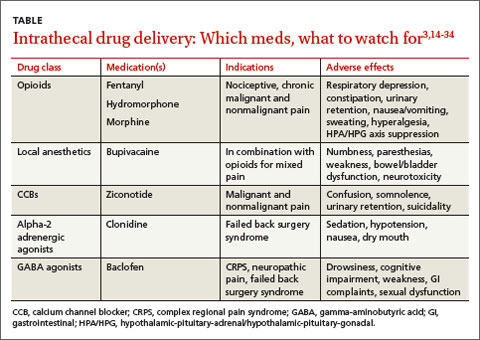
The US Food and Drug Administration (FDA) has approved 3 medications for continuous IT delivery: morphine, ziconotide, and baclofen. But it is common practice to use alternative agents, such as other opioids, local anesthetics, or alpha 2-adrenergic agonists (TABLE).3,14-34
CASE › Ms. G’s primary care physician referred her to a pain specialist, who thought she would benefit from IT analgesia. After a successful single-shot IT trial with 0.5 mg morphine, the patient underwent implantation. The specialist chose morphine as the IT agent because of Ms. G’s history of successful pain relief with it, and because such a low dose was unlikely to be a problem for a patient with renal failure.
A month later, when she returned to the specialist to have the pump refilled, Ms. G reported a pain score of 3.
Opioids such as morphine exhibit a wider spread of analgesia when administered intrathecally, resulting in fewer adverse effects than systemic opioids.13,35,36 The mu-opioid receptors in the dorsal horn of the spinal cord are the primary target of IT opioids.
In a multicenter randomized trial involving 200 cancer patients on opioids, Smith et al4 compared implantable IT drug delivery systems with comprehensive medical management. The mean VAS pain score in the IT group fell 52% vs a decline of 39% in the medical management group.
The evidence supporting IT opioids for nonmalignant pain is not as strong. This may be due to inherent differences in pain mechanisms. In cancer pain, between 75% and 90% of pain is either nociceptive or mixed nociceptive-neuropathic; the etiology of noncancer pain is more variable.37-39
Although IT opioid therapy is associated with a lower incidence of adverse effects than systemic therapy, this route is not devoid of adverse effects. Opioids delivered intrathecally may still be associated with respiratory depression, constipation, urinary retention, nausea/vomiting, sweating, and hyperalgesia.39 In addition, chronic opioid use suppresses the hypothalamic-pituitary-gonadal axis and the hypothalamic-pituitary-adrenal axis14,40,41—a risk with long-term IT as well as systemic administration.14 Respiratory depression most commonly results from accidental overdosing, and patients must be monitored during initiation and dose escalation of IT opioid therapy.15
Local anesthetics. Numerous studies have documented the favorable outcomes of combining local anesthetics with opioids for patients with cancer16-20 and noncancer pain.21,22 Local anesthetics work via the blockade of voltage-gated sodium channels, interfering with neuron depolarization.17
A retrospective study in which patients with malignant pain and those with failed back surgery syndrome had bupivacaine added to their IT opioid solution found that the combination led to lower pain scores and a 23% reduction in opioid dosage.20 In another retrospective review, researchers demonstrated that the coadministration of IT bupivacaine and an opioid decreased the rate of opioid dose escalation by 65% over the first year in patients with noncancer pain.23
However, a double-blind randomized, crossover multicenter study found that in patients with chronic nonmalignant pain, the addition of bupivacaine to IT opioids failed to produce significant improvement in pain control compared with opioid use alone. Quality of life scores did improve, however, in the group receiving combination therapy.24
Adverse effects of local anesthetics delivered intrathecally include numbness, paresthesias, weakness, bowel/bladder dysfunction, and neurotoxicity.17,19,25
Calcium channel blockers. Found in venom produced by the marine snail Conus magus, ziconotide blocks presynaptic N-type channels. It is the only calcium channel blocker used to manage chronic pain.26 Several trials in patients with malignant and nonmalignant pain have shown a significant decrease in VAS pain scores compared with placebo.25,26 In addition, a multicenter, double-blind placebo-controlled crossover study evaluating IT ziconotide for the treatment of refractory pain in 111 patients with cancer and AIDS found that the treatment group obtained significantly better pain relief than the controls (53% vs 17.5% using a VAS pain intensity score).25 However, 31% of those in the treatment group experienced adverse effects, the most common of which were confusion, somnolence, and urinary retention.