THE CASE
A 23-year-old immunocompetent woman was referred to our spinal clinic with a 6-month history of low back pain that radiated to her right flank, buttock, and groin. She’d had intermittent urinary problems, including mild dysuria and frequency, and had been treated with antibiotics for a presumed urinary tract infection on 3 previous occasions, but her pain gradually increased and eventually became constant.
The patient had no history of fever, malaise, or weight loss. She denied consuming unpasteurized milk or undercooked poultry, and hadn’t recently experienced diarrhea or vomiting.
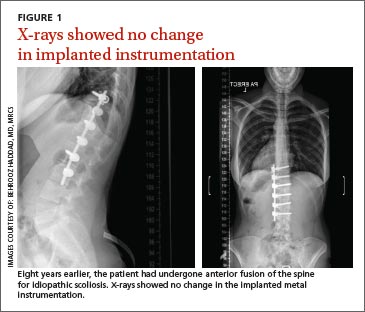
Eight years earlier, she had undergone anterior fusion of her spine for idiopathic scoliosis. At that time, she was at Risser grade 1, and her Cobb angle was 50°; metallic instrumentation was implanted at T10 to L3 to prevent progression of the scoliosis. Her recovery had been uneventful.
During examination, her temperature, pulse, respiratory rate, blood pressure, and nervous system were all normal. Her hips appeared normal, as well, and a straight leg raise was negative bilaterally. The patient had mild midline lumbar tenderness. Spinal range of movement revealed decreased flexion and mild pain.
X-rays (FIGURE 1) showed no changes in the previous metalwork in her spine. There was decreased disk height at the L3/4 level, but no significant bony erosion or soft-tissue shadows. Laboratory testing revealed a C-reactive protein (CRP) level of 240 mg/dL (normal, <1 mg/dL) and her erythrocyte sedimentation rate (ESR) was 102 mm/h—more than 5 times higher than it should have been.1 The patient had a normal peripheral white cell count (WCC). Midstream urine cultures were negative.
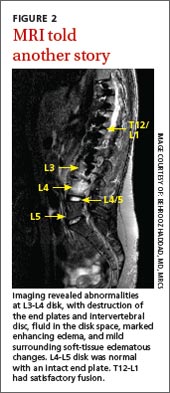
The patient was admitted to the hospital for further work-up. Magnetic resonance imaging (MRI) of the lumbar spine showed gross abnormality at the L3-L4 disk level with erosion of the end plates, fluid in the disk space, marked enhancing edema, and mild surrounding soft-tissue edematous changes, but no evidence of any epidural abscess (FIGURE 2). The patient had a fluoroscopy-guided needle biopsy of the disk on the same day and received intravenous (IV) ceftriaxone 2 g twice a day. Blood and urine cultures were negative.
We suspected our patient had spondylodiscitis, an infection of the spine that includes spondylitis (inflammation of the vertebrae) and discitis (inflammation of the vertebral disk space). After 48 hours, the biopsy sample grew Salmonella typhimurium and confirmed the diagnosis. The organism was sensitive to ceftriaxone and ciprofloxacin; parenteral ceftriaxone was continued and the patient wore a thoracolumbar brace for immobilization. For 3 days, her inflammatory marker levels were checked daily, then every other day for the rest of that first week, and then 2 more times in the following week.
Thoracic and lumbar vertebrae are the most common sites of spondylodiscitis.2 Spondylodiscitis accounts for 3% to 5% of pyogenic osteomyelitis in patients in developed countries.3 The incidence of pyogenic spondylodiscitis may be rising due to an increase in the number of elderly and immunocompromised patients, as well as a rise in invasive medical procedures.4-6
If left untreated, spondylodiscitis can spread longitudinally (involving the adjacent levels), posteriorly (causing bacterial meningitis, abscess formation, and cord compromise), or anteriorly (causing paravertebral abscess). Untreated spondylodiscitis can also send distant infective emboli and cause endocarditis7-9 or mycotic abdominal aneurysm.10
Historically, mortality in patients with vertebral osteomyelitis has been as high as 25%.11 The combination of earlier diagnosis, antibiotics, and surgical debridement and stabilization has decreased mortality to less than 15%.12-14
Risk factors for spondylodiscitis include male sex, IV drug abuse, diabetes, morbid obesity, having had a genitourinary or spinal procedure, and being immunocompromised (eg, from alcohol abuse, malignancy, organ transplantation, chemotherapy, or corticosteroid use).12,15,16
Gram-positive organisms cause most spine infections in both adults and children, with 40% to 90% caused by Staphylococcus aureus.17 Gram-negative organisms (Escherichia coli, Pseudomonas, and Proteus), which can also cause spondylodiscitis, typically occur after genitourinary infections or procedures. IV drug abusers are prone to Pseudomonas infections.18 Anaerobic infections may be seen in patients with diabetes or after penetrating trauma.15 Salmonella species can cause spondylodiscitis, especially in patients with sickle cell disease from an intestinal source.19
Mycobacterium tuberculosis is the most common nonpyogenic infecting agent that also can cause spondylodiscitis. Infection caused by tuberculosis (TB) has had a recent resurgence with resistant strains, especially in patients with human immunodeficiency virus.15 Although less than 10% of patients with TB have skeletal involvement, 50% of the skeletal involvement occurs in the spine.15
The clinical presentation of spondylodiscitis depends on the location of the infection, the virulence of the organism, and the immune status of the patient. Discitis can present as pain in the back, hip, abdomen (especially in children20) and, occasionally, with meningeal involvement.11 Patients with discitis often have a normal temperature.15,21 In patients with discitis, the patient’s WCC will be normal, but the ESR is almost always elevated.15,22 Suspect spondylodiscitis in patients who present with persistent or increasing pain 3 to 4 weeks after back surgery. For such patients, measure inflammatory markers and order imaging of the spine.