Introduction
Between 2006 and 2013, over 9,000 continuous flow left ventricular assist devices (LVADs) were implanted in patients with end-stage heart failure; nearly 2,500 of these devices were placed in 2013 alone.1 As the number of patients with an LVAD continues to grow, so too does the likelihood of a patient with an LVAD presenting to the ED—even if the hospital is not a designated VAD center. An earlier article appearing in the February 2014 issue of Emergency Medicine addressed the management of the unique medical complications faced by patients with LVADs.2 This article focuses on troubleshooting the device when a patient with a LVAD presents to the ED.
Device Indications and Types
Left ventricular assist devices are mechanical implantable devices that provide circulatory support to patients with refractory advanced heart failure. A few of these devices are approved by the US Food and Drug Administration for use as either a bridge to heart transplant or as destination therapy if the patient is not a candidate for heart transplant.
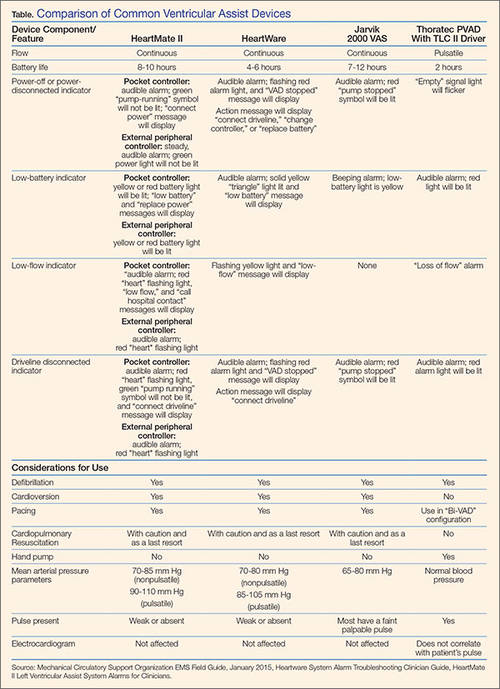
Nearly all of the LVADs currently on the market are designed to provide continuous flow.3-6 The most commonly employed LVADs include the HeartMate II (Thoratec Corporation, Pleasanton, California), HeartWare Ventricular Assist System (HeartWare, Framingham, Massachusetts), and the Jarvik 2000 VAS (Jarvik Heart, New York, New York) (Table). These devices differ somewhat in configuration, but the initial management of LVAD patients with a device malfunction is essentially the same.
Even though the type of device is clearly marked on the patient’s controller, to ensure appropriate management and facilitate troubleshooting for malfunction, patients should always carry an information card identifying the type of device implanted, as well as the complete contact information for each of their health care providers, including their LVAD coordinator.3,7
Device Components
Left ventricular assist devices consist of several different components. All LVADs consist of a pump, controller, driveline, and batteries/battery pack that work together to augment function of the native heart.
Pump
The LVAD pump is surgically implanted into the patient’s abdominal or chest cavity, with an inflow cannula positioned in the left ventricle and an outflow cannula inserted into the ascending aorta. The pump is designed to have a single internal moving part called the impeller. The pump draws blood from the left ventricle and directs it to the aorta.
Controller and Driveline
The actions of the pump are directed by a controller, a mini-processor contained in a small box located outside the patient’s body. This processor is connected to the pump by a driveline inside the body. The driveline exits the body through the patient’s abdominal wall and connects to the controller. The controller regulates the pump speed and provides information about pump speed, flow, pulsatility index, and power of the LVAD.3,4
Speed Monitor. The LVAD speed on the controller is usually set at the time of discharge from the hospital; most devices cannot be changed manually.
Power Monitor. On the monitor, the "power" indictor reflects the voltage and current of the pump motor, whereas the "flow" indicator is a reflection of both power and speed (ie, the higher the power, the higher the flow and vice versa).
Batteries/Battery Pack. The LVAD is powered by two batteries attached to the controller or, in some models, to a power base unit that can be plugged into an electrical outlet. Each battery is connected to the controller by a separate connector wire. When battery power in the device becomes low, the batteries should be replaced with fully charged backup batteries, one battery at a time. If the controller is disconnected from both batteries at the same time, the LVAD will lose power and stop working. It is critical to patient health that the LVAD be powered at all times.3,5,7,8
Pulsatility Index. Changes in a patient’s blood pressure (BP) can affect flow, with higher BP causing a decrease in flow. The pulsatility index reflects the heart’s contractility and stretch, as well as the patient’s volume status. As the preload decreases (ie, due to a decrease in blood volume) the device will indicate a decreased pulsatility index. If the patient is volume overloaded, the pulsatility index will be increased. Pump speed and pulsatility index are inversely related. In some devices, if the controller detects a significant change in pulsatility index from the prior 15-second average, it will reduce the pump speed to low and then gradually accelerate to the set fixed speed.3,8 Significant changes in pulsatility index often indicate an event has occurred, such as an obstruction of the inflow cannula, a decrease in the patient’s volume status, an arrhythmia, or increased pulmonary artery pressure suggestive of right heart failure.3,4