NAPLES, FLA. – Partial repair of flail segment rib fractures may suffice in patients whose anatomy precludes full stabilization, a small study suggests.
After a median follow-up of 189 days, only predicted total lung capacity at 3 months (90% vs. 72%; P = .02) and 6 months (94% vs. 75%; P = .038) significantly differed between patients undergoing complete flail stabilization (CFS) vs. partial flail stabilization (PFS).
No other differences in pulmonary and clinical outcomes were observed between the 43 patients, Dr. Terry P. Nickerson reported at the annual scientific assembly of the Eastern Association for the Surgery of Trauma.
 Courtesy Dr. Brian Kim
Courtesy Dr. Brian Kim
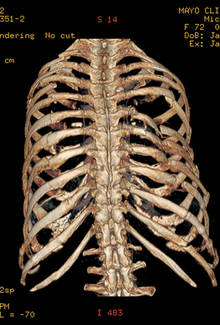
X-ray of a woman who was trampled by a horse. CT Chest, 3 dimensional reconstruction. Bilateral flail chest left 2-10 and right 4-11. Note the cavitary right chest flail segment.
Flail chest is defined by two or more consecutive ribs fractured in two places and a segment of chest wall unable to contribute to respiratory mechanics.
Benefits of surgical stabilization of flail chest reported in the heterogeneous literature include decreased ICU stay, lower rates of pneumonia, increased return to work, improved quality of life, and low surgical morbidity, Dr. Nickerson noted.
The retrospective analysis, included all patients (aged 30-85 years) who underwent surgical rib fracture stabilization for flail chest from August 2009 through February 2013 at the Mayo Clinic Hospital, St. Marys Campus, Rochester, Minn. In all, 23 patients had CFS, defined as all fractures involved in a flail segment undergoing full fixation, and 20 had PFS or at least one flail segment not completely repaired.
The CFS and PFS groups were similar with respect to median age (63 years vs. 58 years), sex (52% male vs. 65% male), operating time (186 minutes vs. 183 minutes), Injury Severity Score (20 vs. 17), hospital length of stay (10 days for both), ICU stay (1 day vs. 2 days), and narcotic use at 1-month follow-up (50% vs. 47%), according to the poster presentation.
At 6 months, there were no significant differences between the CFS and PFS groups in predicted vital capacity (86% vs. 76%), forced vital capacity (85% vs. 77%), forced expiratory volume in 1 second (71% vs. 78%), and FVC/FEV1 ratio (68% vs. 74%).
Rates of pneumonia were also similar in the two groups (21% vs. 20%; P = .39), reported Dr. Nickerson, a general surgeon in Rochester.
No patient or provider observed a significant chest wall deformity in either group during follow-up and no reoperations were required for incomplete repair in the PFS.
 Courtesy Dr. Brian Kim
Courtesy Dr. Brian Kim
Postoperative CXR following bilateral multilevel flail chest stabilization - stabilization of right ribs 5-9 with flail bridged 6-8, stabilization of left ribs 3-9 with posterior elements of flail stabilized.
"Despite advances in surgical technique, not all flail segment rib fractures are accessible for repair via standard thoracotomy," the authors wrote. "Our data suggest that PFS is acceptable and that extending or creating additional incisions for exposure for CFS is unwarranted."
Additional research assessing late complications, performance/functional outcomes, and perceived benefits of the operation is needed to determine whether partial repair is truly comparable with full stabilization, coauthor Dr. Brian Kim, associate medical director Mayo Clinic Trauma Center, Rochester, said in an interview.
In their experience, 6 months’ postoperative follow-up has been sufficient with respect to bony healing, convalescence from pain, and monitoring of chest wall integrity.
He noted that some surgeons may be dissuaded from pursuing or recommending operative stabilization of a flail segment with fractures deemed outside the boundaries of repair, particularly if the injury is in the elderly or obese patient.
"The results of our study lend support to the practice of repairing the most anatomically disrupted and/or symptomatic fractures within the flail segment," he said. "Age and/or BMI [body mass index] are not absolute contraindications for flail segment stabilization in our practice."
Poster session moderator Dr. Alexander Eastman of University of Texas Southwestern Medical Center in Dallas, said the low patient numbers and short follow-up in the study make it difficult to draw big conclusions, other than the need for further research.
His group uses surgical fixation of flail chest for patients with instability and pain management for those patients who are difficult to wean from the ventilator.
"I think many surgeons still are skeptical of the data supporting fixation of flail chest," he noted in an interview.
Dr. Nickerson and his coauthors reported having no financial disclosures.