Etiology of Respiratory Failure and Treatment Decisions
At the time of initial presentation, the exact etiology of a patient’s respiratory failure may not be known, and treatment decisions will be necessary before all relevant data are present. Patients presenting in acute respiratory distress (ARD) are often suffering from shunt physiology, in which alveoli are perfused but not ventilated due to the presence of fluid or collapse, as in pulmonary edema or COPD.4 Regardless of the etiology, patients will benefit from early application of NIV.5 Thus, the clinician must be aggressive in the application of this therapy to identify those patients who will benefit the most from treatment. All patients receiving NIV must be monitored closely as failure of therapy is still a possibility.
Patient Selection
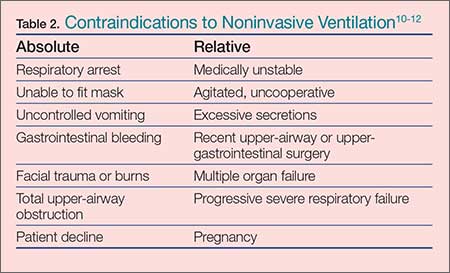
The utilization of NIV has increased in the hospital and ED setting and it is now often initiated in the prehospital setting6-8 with observed improvement in dyspnea scores and oxygenation with early intervention.9 Regarding patient selection, in the absence of contraindications (Table 2), all dyspneic patients should be considered eligible for a trial of NIV. 13 For some patients, this may be their first use of the therapy; as such, they are in effect learning to “swim while drowning.” The agitated and anxious patient will require coaching to provide reassurance and instruction while he or she learns to synchronize and work with the ventilator. The presence and quality of this instruction, though not previously measured, would intuitively be very helpful and an important determinant of success in the application of NIV in the naïve patient.
Common Conditions and NIV
In the ED, NIV is commonly utilized for the treatment of COPD and acute decompensated heart failure. These two conditions have been extensively studied and a robust amount of literature supports the routine use of NIV in these patients.
Chronic Obstructive Pulmonary Disease
For COPD, BiPAP has been shown and is widely accepted as the modality that confers the most benefit, with one study demonstrating a 462% increase in its use and a 42% decline in mechanical intubation rates from 1998 to 2008.14 Multiple studies have demonstrated a reduction in the intubation rate, improvement in the work of breathing, and a more rapid improvement in RR and symptoms.15,16
Acute Decompensated Heart Failure and Pulmonary Edema
Noninvasive ventilation is used commonly for decompensated heart failure and acute cardiogenic pulmonary edema (ACPE). The rapid patient improvement with its use when compared to standard O2 therapy is well documented. A successful trial and application of NIV demonstrated benefit in a recent retrospective analysis of 2,430 acutely decompensated heart-failure patients in the United States. The study found that the patients who were treated with NIV, but not immediately intubated, had better outcomes.17 (In these types of patients, pulmonary edema is typically not related to volume overload, but the result of imbalanced hemodynamics with markedly increased cardiac afterload and systemic vascular resistance.)
With respect to type of NIV, the use of CPAP is widely accepted as the primary modality of choice to confer the most benefit in ACPE.18 Although theoretical advantages do exist for the use of BiPAP over CPAP, this benefit has been noted in smaller studies19 but not clearly demonstrated in large reviews.20,21 In addition, patients suffering from long-term CHF develop the syndrome of cardiac cachexia, characterized by the loss of quantity and quality of skeletal muscle.22 This reduction in muscle mass can produce a significant deficit in inspiratory muscle strength and ability, providing an opportunity for benefit with the use of BiPAP.
Previously, BiPAP was considered unsafe in the setting of ACPE due to an increase in myocardial infarction.23 These results have not been reproduced in larger studies, and it is widely accepted that although BiPAP may not confer any benefit, it also does not increase harm.
Asthma
Because the underlying pathology of asthma differs from COPD, the current evidence for NIV use in patients presenting with an asthmatic episode is not very strong. Chronic obstructive pulmonary disease is characterized by collapse of terminal airways, with destruction of pulmonary architecture, and decreased compliance of the chest wall. In contrast, the airway obstruction in asthma progresses as the severity of the attack increases, and NIV may offer potential benefit in high-risk patients to avoid intubation.24 Several small studies suggest the application of NIV for severe asthma exacerbations is reasonable, with some demonstration of improvement in the work of breathing and ventilatory status.25-27
The Critically Ill Patient
Critically ill patients represent a high-risk group for desaturation during endotracheal intubation, and NIV should be considered for preoxygenation unless contraindications exist (Table 2). If standard high-flow O2 without positive pressure does not improve oxygenation, the application of NIV may overcome shunt physiology, improve oxygenation, and lessen peri-intubation time with dangerous desaturation events.4,28-30