BARCELONA— Risk calculators are usually confined to certain populations, but the recently updated ACC/AHA calculator might be effective beyond the United States borders in a Southern European population.
Researchers from Portugal compared the ACC/AHA risk calculator to the European Systematic COronary Risk Evaluation (SCORE) in a patient population that was treated with lipid-lowering drugs. They found that the ACC/AHA calculator’s cut-off point at 7.5% was "extremely effective in discriminating high-risk subject," said Dr. Manuel Oliveira-Santos of Coimbra (Portugal) University, who presented the findings at the annual congress of the European Society of Cardiology.
They also found that that the two scoring systems were strongly correlated and well calibrated. Both calculators overestimated the cardiovascular (CV) risk, "which confirms the previous findings and shows that the calculator works, since many patients in the study were treated with statins," said Dr. Kim A. Williams Sr., president-elect of the American College of Cardiology, who was not involved in the study.
One of the main differences between the two calculators is that the ACC/AHA risk calculator predicts atherosclerotic cardiovascular disease (ASCVD) events, while SCORE estimates the individual risk of fatal noncoronary atherosclerotic and coronary heart disease only, said Dr. Oliveira-Santos.
The study's primary endpoint was acute myocardial infarction, stroke and CV death at 10 years, and the aim was to find out if the ASCVD could be a meaningful tool for this particular patient population in Portugal, said Dr. Oliveira-Santos.
The team retrospectively calculated the two scores for 446 CV-naive patients who were treated at a lipidology clinic between 1994 and 2007. Patients were divided to four groups according to the ASCVD (cut points at 5%, 7.5%, and 10%) and the SCORE system (cut points at 1%, 5%, and 10%).
The mean age of the population was 49 years; more than half were men; 21% were smokers, 25% had type 2 diabetes. More than half were on antihypertensive drug therapy and 72% were receiving statin treatment.
Researchers were able to follow up 85% of the patients at 10 years. Of those, 3.4% had an acute MI, 2.4% had a stroke, and 1.5% died of a cardiovascular event.
The median calculated CV death risk based on SCORE was 0.95%, and the median CV risk calculated by ASCVD was 8.5%. The observed event rate based on the SCORE definition was 1%, compared to 6% based on the ASCVD definition.
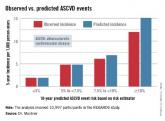
When ASCVD was applied to the study cohort, the majority of the patients fell at the very low (less than 5%) or very high (10% or higher) risk categories. About 20% of the patients were at medium risk categories.
Patients who fell in the low and very low risk categories – in other words, they had a CV risk of less than 7.5% – had – no actual cardiovascular events. In the 10% or higher risk group, the predicted event rate was nearly twice the observed rate.
The overestimation, especially in the low risk category (5% to 7.5%) could lead to unnecessary statin therapy and may raise some safety concerns, but the overestimation in the high-risk category is not problematic, Dr. Oliveira-Santos said.
Meanwhile, the group at medium-high risk (from 7.5% to less than 10%) had a slightly higher rate of actual CV events than that estimated using the calculator. "We don’t see that as a cause for concern since those are high risk patients in whom statin therapy is indicated. The statin-treated patients in our study are the majority," he said.
When the SCORE calculator was applied to the cohort, the CV death risk was overestimated in all groups. The majority of the patients fell in the very-low- or low-risk categories, and there were no CV deaths in the very-low-risk category, which included 51% of the patient population.
Researchers conducted further analysis and found that the SCORE and ASCVD systems were positively correlated and they both had "good and similar discriminative power," in addition to good calibration, Dr. Oliveira-Santos reported.
Dr. Williams said that the correlation of the two systems is good news. "There’s always going to be interest in how well an American score will predict the risk in a European population. And the fact that there’s good correlation is reassuring.
"And the most important thing is whether or not an individual practitioner in another country should feel comfortable using this calculator, and that’s why we need more of this kind of study — to find out if they need to build another application or whether they can use what we’ve already created," said Dr. Williams, professor and chief of cardiology at Rush University in Chicago.