Dr. Krefft is a resident, Dr. Nawaz is an associate professor, and Dr. Miller is a professor of medicine, all at the University of Colorado Anschutz Medical Campus in Aurora. Dr. Rose is also an associate professor at the University of Colorado in Denver. Dr. Miller and Dr. Nawaz are also physicians at the VA Eastern Colorado Health Care System in Denver.
The patient joined the Army National Guard in 2006 and was activated in 2009 to deploy to Afghanistan from January 2010 through January 2011. She was stationed at Bagram Airbase for the entire deployment and worked as a military police officer in the prison. She had exposure to sandstorms and burn pit combustion products. The prison was about 2 miles downwind from a large burn pit.
In October 2010, she quit smoking again because of new-onset chest tightness and dyspnea on exertion. However, her symptoms did not abate, and she noted increased chest tightness and difficulty catching her breath when running near the burn pit. While she tried to avoid the burn pit, she participated in competitive races and a 10-mile run along paths that were near the burn pit.
After returning from deployment, the patient presented to her VA PCP for evaluation of persistent nonproductive cough, chest tightness, and dyspnea on exertion. She was not taking any respiratory or allergy medications at the time of evaluation. Initial chest X-ray and spirometry were normal, and she was referred to the chest clinic for consultation. At the time of pulmonary consultation, the patient had a total smoking history of 15 pack-years but had now abstained from smoking for about 2 years. She reported residential exposure to pet birds for > 20 years. High-resolution chest imaging and full PFT with lung volumes and diffusion capacity were performed to evaluate for hypersensitivity pneumonitis.
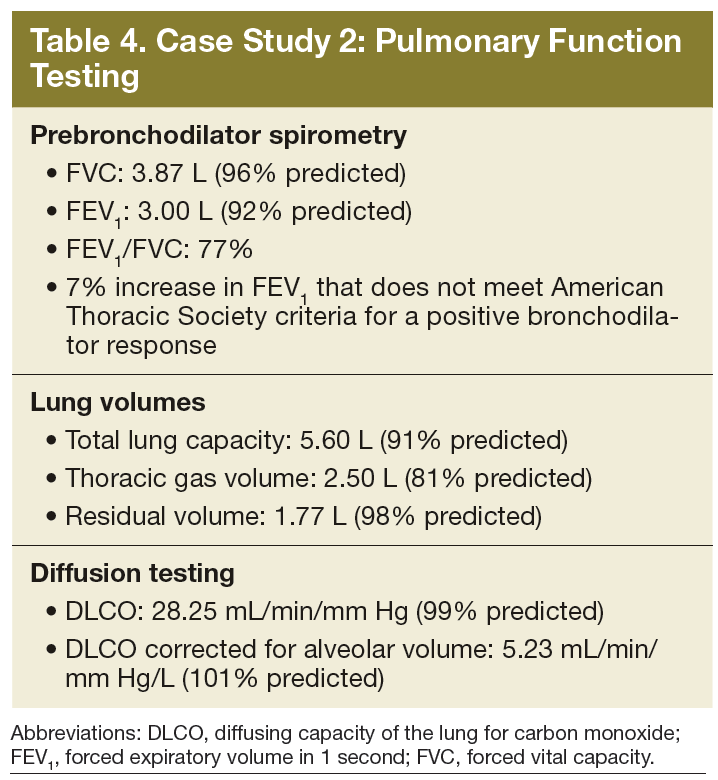
Her vital signs, physical examination pulmonary function testing with spirometry, lung volumes, and diffusion testing were all normal (Table 4). Bronchial challenge to methacholine demonstrated airways hyperresponsiveness at a PC[-20] FEV 1 of 1.25 mg/mL. High-resolution chest CT did not demonstrate air trapping, centrilobular nodules, or other evidence of chronic interstitial lung disease. A cardiopulmonary maximum multistage exercise test with arterial line placement showed normal exercise tolerance with the patient achieving 109% of the maximum predicted workload and 90% of predicted VO 2 max.
The patient was diagnosed with deployment-related asthma based on the finding of airways hyperresponsiveness after bronchial challenge testing. Her asthma was considered deployment-related based on the temporal onset of cough and later chest tightness and dyspnea on exertion that occurred during deployment. Ongoing smoking cessation was emphasized.
The patient was started on bronchodilator therapy with albuterol prior to exercise and as needed, but she continued to have symptoms of chest tightness while exercising. Eventually, a low-dose ICS was initiated in conjunction with albuterol as needed. Her symptoms did not resolve with this regimen, but she did experience improvement in exertional chest tightness. This patient was not referred for biopsy given clinical findings of asthma. She will continue pulmonary monitoring every 6 months. However, if her symptoms worsen, she will undergo full PFT, which includes lung volumes and diffusion testing and possible repeat chest imaging.
Conclusion
These 2 cases are representative of the spectrum of deployment-related lung disease. This assessment requires a detailed chronologic occupational and environmental history, establishing a temporal link between respiratory symptoms and deployment exposures and evidence of lung disease on noninvasive testing (or confirmation by surgical lung biopsy in select cases) in which noninvasive testing is nondiagnostic.