Dr. Tardi, Dr. Kapadia, and Dr. Kurpius are clinical pharmacy specialists at the Jesse Brown VAMC and clinical assistant professors at the University of Illinois-Chicago College of Pharmacy, all in Chicago, Illinois. Dr. Fairbanks is a mental and behavioral health psychologist and Dr. Foglio is a PGY-1 pharmacy practice resident, both at the Jesse Brown VAMC.
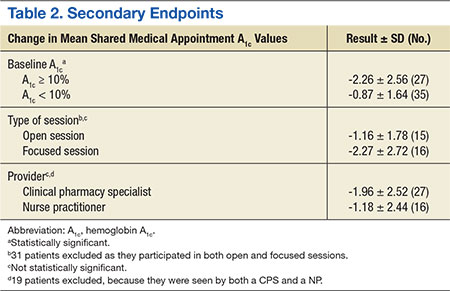
For the primary endpoint, the SMA group had a 1.48% ± 0.02 (SD) reduction in A 1c compared with a 0.6% ± 0.02 (SD) decrease in the control group ( P= .01). When evaluating mean changes in A 1c by the number of SMAs attended, it was noted that participation in ≥ 6 SMAs led to the greatest reduction in A 1c of 2.08%. In the SMA group, it was noted that patients with higher A 1c values at baseline demonstrated greater improvements in glycemic control compared with patients with lower baseline A 1c values. The mean change in A 1c, stratified by baseline A 1c, was -2.26% for those with baseline A 1c values ≥ 10% and -0.87% for those with baseline A 1c values < 10%.
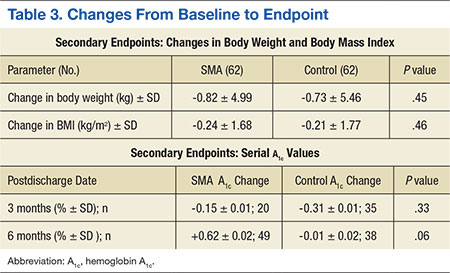
In evaluating the format style, open- vs focused-session, it was observed that participation in focused sessions led to greater improvements in glycemic control. Furthermore, when stratified by provider, greater improvements in glycemic control were demonstrated when medication management was completed by a CPS vs a NP (Table 2). The average number of interventions per SMA patient was 3.1 ± 2.22 (SD). For the control group, the total number of interventions made was 86, with an average of 1.37 ± 1.51 (SD) per patient. The overall show rate was 49% ± 16 (SD), 52% ± 16 (SD) for open visits, and 46% ± 15 (SD) for focused visits. The mean change in ABW and BMI from baseline to endpoint was no different between the SMA and control groups (Table 3). The SMA group participants demonstrated a decrease in A 1c at 3 months postdischarge, and a moderate increase in A 1c was noted at 6 months postdischarge.
Discussion
Shared medical appointments provide an effective alternative to standards of care in order to obtain improvements in glycemic control. Consistent with previous studies, this study reported significant improvements in glycemic control in the SMA group vs the control group. This study also elucidated unique characteristics about SMAs that may have been correlated with clinical success.
Although the greatest improvements in glycemic control were noted for those who participated in ≥ 6 SMAs, it was observed that participation in only 1 SMA also led to improvements. For a site with limited staff and a high volume of patients waiting to participate in SMAs, it may be mutually beneficial to offer only 1 SMA per patient. In addition, patients with ≥ 10% A 1c at baseline demonstrated greater improvements in glycemic control compared to those with < 10% A 1c at baseline. The reasons the higher baseline A 1c subgroup responded to interventions more robustly are unclear and likely multifactorial. Nonetheless, factors such as psychosocial influences (eg, peer pressure to get healthy) may have increased motivation to prevent complications and improved medication adherence in the setting of closer follow-up. Additionally, hyperresponsiveness to drug therapy may have played a role. Regardless, for new SMA programs interested in making an immediate impact, it may be advantageous to initially select patients with very poorly controlled DM.