Ms. Archambault is a social worker in the Department of Geriatrics and Palliative Care; Ms. Doherty and Ms. Kelly served as research assistants within the Geriatric Research Education and Clinical Center at the time the article was written; Ms. Doherty is currently a research assistant, all at the VA Boston Healthcare System in West Roxbury, Massachusetts. Dr. Rudolph is the director of the Center of Innovation in Long-Term Services and Supports at the Providence VA Medical Center in Rhode Island. Ms. Kelly is currently working as a nurse and completing her training as a nurse practitioner candidate.
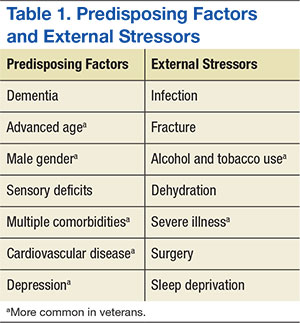
Predisposing factors for delirium, such as age and sex, lifestyle choices (alcohol, tobacco), and chronic conditions (atherosclerosis, depression, prior stroke/transient ischemic attack) are more prevalent in the veteran population. 9,17-20 In 2011, the median age for male veterans was 64 and the median age for male nonveterans was 41. Of male veterans, 49.9% are aged ≥ 65 years in comparison with 10.5% of the nonveteran male population. 21 Veterans also have higher rates of comorbidities; a significant risk factor for delirium. 20 A study by Agha and colleagues found that veterans were 14 times more likely to have 5 or more medical conditions than that of the general population. 9 In a study comparing veterans aged ≥ 65 years with their age matched nonveteran peers, the health status of the veterans was poorer overall. 22 Veterans are more likely to have posttraumatic stress disorder, which can increase the risk of postsurgery delirium and dementia, a primary risk factor for delirium. 23-26
Delirium Intervention
Up to 40% of delirium cases can be prevented. 27 But delirium may remain undetected in older veterans because its symptoms are sometimes thought to be the unavoidable consequences of aging, dementia, preexisting mental health conditions, substance abuse, a disease process, or the hospital environment. 28 Therefore, to avoid the negative consequences of delirium, prevention is critical. 28
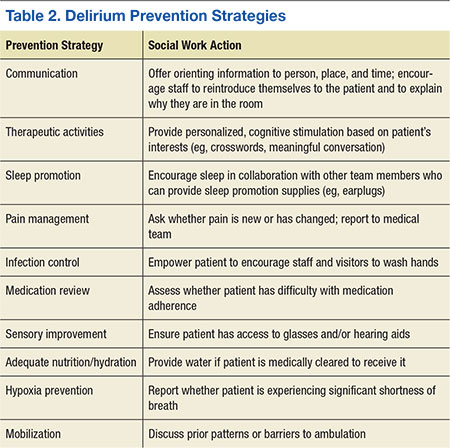
The goals of delirium treatment are to identify and reverse its underlying cause(s). 29 Because delirium is typically multifactorial, an HCP must carefully consider the various sources that could have initiated a change in mental status. Delirium may be prevented if HCPs can reduce patient risk factors. The 2010 National Institute for Health and Clinical Excellence (NICE) Delirium Guideline recommended a set of prevention strategies to address delirium risk factors (Table 2). 12
As a member of the health care team, social workers can help prevent delirium through attention to pain management, infection control, medication review, sensory improvement, adequate nutrition and hydration, hypoxia prevention, and mobilization. 12No pharmacologic approach has been approved for the treatment of delirium. 30 Drugs may manage symptoms associated with delirium, but they do not treat the disease and could be associated with toxicity in high-risk patients. However, there are a variety of nonpharmacologic preventative measures that have proven effective. Environmental interventions to prevent delirium include orientation, cognitive stimulation, and sensory aids. A 2013 meta-analysis of 19 delirium prevention programs found that most were effective in preventing delirium in patients at risk during hospitalization. 31 This review found that the most successful programs included multidisciplinary teams providing staff education and therapeutic cognitive activities. 31 Social workers can encourage and directly provide such services. The Delirium Toolbox is a delirium risk modification program that was piloted with frontline staff, including social workers, at the VA Boston Healthcare System in West Roxbury, Massachusetts, and has been associated with restraint reduction, shortened length of stay (LOS), and lower variable direct costs. 32
Social Worker Role
Several studies, both national and international, have indicated that little has been done over the past 2 decades to increase the diagnosis of delirium, because only 12% to 35% of delirium cases are clinically detected within the emergency department and in acute care settings. 33-37 Patients may hesitate to report their experience due to a sense of embarrassment or because of an inability to describe it. 38