Balance
Balance is a complex skill based on the interaction of dynamic sensorimotor processes. Balance maintains postural control by keeping the body mass (center of gravity) centered on its support base during stance or voluntary dynamic movements and involves regaining stability quickly in response to destabilizing external perturbations. Balance is preserved by postural motor response adjustments to internal and external forces and environmental stimuli.
Balance is classified as either static, maintaining a base of support with minimal movement, or dynamic, maintaining a stable base of support while completing a purposeful movement. Visual, vestibular, and somatosensory signals are sent to the central nervous system, which in turn adjusts body sway and posture by integrating this information and by controlling skeletal muscles to perform appropriate responses for balance. The brain regions involved in gait control include the premotor cortex and parietal lobes.12
Sustaining postural control is critical for the successful and safe performance of most daily activities. Postural instability occurs particularly in elderly individuals due to any combination of decreased sensitivity in sensors, less effective sensory information input to the central nervous system, and reduced muscular capacity. Patients respond to the majority of postural perturbations through movement primarily at the ankles and hips, called the ankle and hip strategy.
The ankle strategy is most effective for countering slow, smaller perturbations. This requires sufficient ankle range of motion and strength to help maintain stability. The ankle muscles and joint receptors also provide proprioceptive information that assist in the correction of postural sway. When larger external forces are applied during stance, postural control of the body relies more on the hip muscles (hip strategy) as opposed to the ankle muscles. The hip flexor and extensor muscles act during the single-limb stance portion of gait and throughout dynamic turning. Thus, weakness in these muscles contributes to instability during gait and dynamic activities. Larger perturbations trigger a stepping strategy to regain postural control.
Stepping strategy involves an attempt to reestablish a new base of support by stepping forward or backward when the center of gravity has exceeded the original base of support. In the elderly, deficiencies of neural input, environmental feedback, central nervous system sensory integration, and motor output lead to impaired balance and falls. Rehabilitation efforts aim to improve the efficiency and integration of the sensory and motor systems.13-19
By addressing balance and postural instability and associated muscular weakness, vestibular-trained PTs are integral to mitigating fall risks and concomitant fall-related injuries in the aging elderly population.
Implementation
The Gait and Balance CVT pilot was approved as an exempt protocol by the NF/SGVHS VA Research and Development Committee and the affiliated University of Florida Institutional Review Board.
A technician at the Gainesville division scheduled a 1-hour appointment for both the outpatient clinic and main hospital clinic. The appointment duration for a face-to-face encounter was the same as the CVT appointment. At the remote site, medical support staff assisted veterans with appointment check-ins, and a telehealth certified technician (TCT) escorted veterans to the examination room for the CVT visits.
The PT’s office had two 18-inch dual computer monitors. One monitor was for the Computerized Patient Record System (CPRS), and the other was for the CVT visit. The PTV’s computer had a speaker with a webcam that panned in or out at the remote site. The webcam’s software was preinstalled. The outpatient clinic examination room is 18 x 20 feet, accommodating various physical examination testing maneuvers.
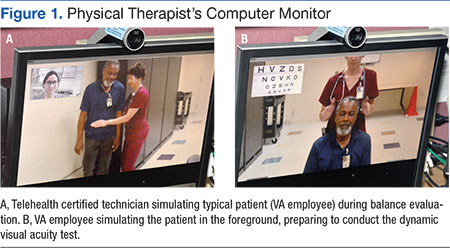
In the examination room, the TCT accessed a telehealth mobile cart with a preinstalled webcam and speakers. This cart also connected peripheral devices, such as a stethoscope or otoscope (Figures 1A and 1B). The basic webcam cost about $120. The remote site telehealth mobile cart cost ranged from $30,000 to $45,000 per unit, depending on the complexity. The mobile cart can be used for a variety of specialty CVT visits. The VA purchased a software license for the webcam and cart-attached computers.
One of the project’s implementation