Asthma is a chronic inflammatory disorder of the airways that leads to airflow obstruction and bronchial hyperresponsiveness. Clinical features of asthma include episodic cough, wheeze, and dyspnea, which may resolve with avoidance of triggers or therapy. Characteristic triggers of asthma are irritanttype airway exposures, including cold air, exercise, various environmental allergens, and work-related exposures. Work-related exposures are the etiology for occupational asthma and work-exacerbated asthma, accounting for up to 25% of adult-onset asthma. 1 It is imperative that clinicians evaluate the clinical history, pulmonary function testing, and response to prior therapies when caring for patients with asthma.
Asthma is common in active-duty service members, despite the diagnosis limiting entrance into the military, and there is potential for significant rates of underdiagnosis among new recruits. 2 Recent changes in military medical guidelines have allowed service members with well controlled asthma to remain on active duty. 3 This potentially increases the number of service members with compromised respiratory status, which is concerning in light of the past decade of deployment to southwest Asia (SWA) and ongoing investigations into potential deployment-related irritant respiratory exposures.
Diagnosis
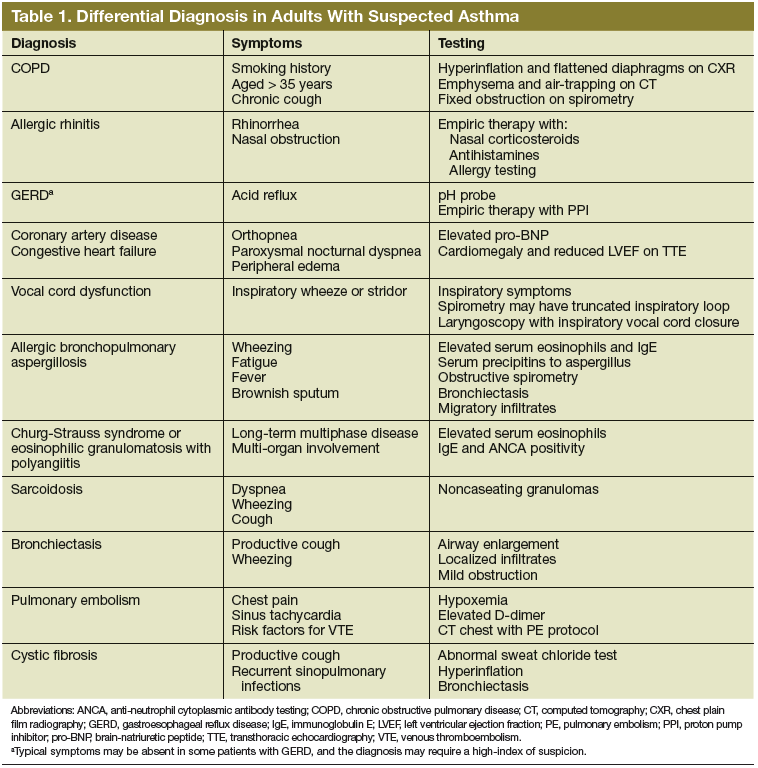
An accurate initial diagnosis is a critical starting point in the management of asthma. Many diseases can mimic asthma, including vocal cord dysfunction, chronic obstructive pulmonary disease (COPD), congestive heart failure, sarcoidosis, allergic bronchopulmonary aspergillosis
(ABPA), and eosinophilic granulomatosis with polyangiitis (EGPA), formerly known as Churg-Strauss syndrome (Table 1). 4 Asthma-mimics, in particular ABPA and EGPA, are often diagnosed via careful longitudinal follow-up.
Characteristic symptoms of asthma include cough, wheeze, dyspnea, chest tightness, and sputum production. Symptoms should be described systematically in terms of onset, frequency, duration, diurnal variability, and seasonality. A careful review of systems should be conducted to exclude conditions such as COPD, pulmonary emboli, congestive heart failure, viral syndromes, acute infection, or hypersensitivity pneumonitis. Patients must be queried (carefully and often repeatedly) about potential triggers, including physical activity, hobbies, pets (including any animals owned by the patient, family members, or living on the property), and occupation.
Physical examination may reveal presence of nasal polyps, nasal mucosal swelling, increased secretions, wheezing, a prolonged expiratory phase, atopic dermatitis, or eczema. Further cardiac evaluation with transthoracic echocardiography may be considered in patients with a heart murmur. Digital clubbing is not characteristic of asthma and should prompt investigation of alternative inflammatory disease (connective tissue disease, interstitial lung disease, or bronchiectasis).
Pulmonary function testing including spirometry and bronchodilator response should be performed as demonstration of airflow limitation is crucial for the diagnosis of asthma. 4 Spirometry should be performed in accordance with published standards and documented in the patient's medical record. Airflow limitation should be described in accordance with the Third National Health and Nutrition Examination Survey (NHANES III) references values as recommended by the American Thoracic Society and the European Respiratory Society (ATS/ERS) guidelines. 5-7 Obstruction is defined as an forced expiratory volume in 1 second to forced vital capacity (FEV1/FVC) ratio less than the fifth percentile of the
normal distribution (lower limit of normal). Bronchodilator testing should also be performed to establish presence and degree of response to inhaled bronchodilator medication. A12% increase in the FEV1 with an absolute increase of 200 mL is considered significant in adults. 7