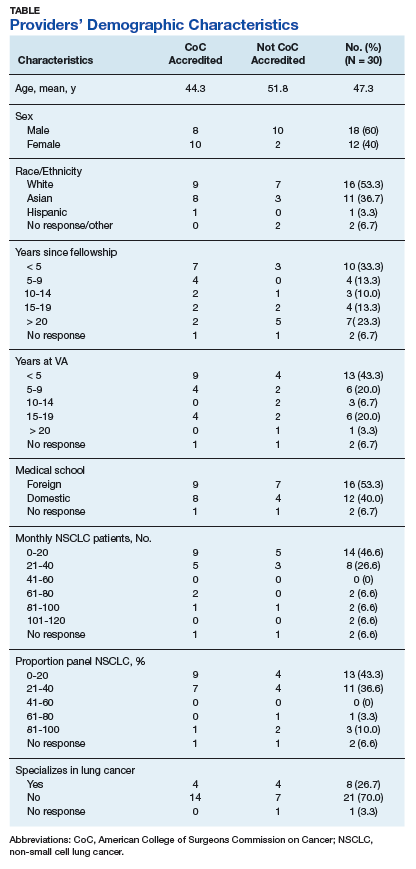
Thirty medical oncologists were interviewed. Participant demographics are presented in the Table.
Barriers to testing
The 2 most commonly cited barriers to ordering mutation testing can be considered weaknesses in the testing process: lack of tissue and wait time for results. Almost all providers identified lack of tissue as a barrier to ordering a mutation test.
Another frequently cited testing weakness involved the wait time for results. Because the mutation analysis is not conducted in the VHA facility, providers often must wait 2 to 4 weeks to receive results. This can present a problem because some providers do not want to wait for the results before recommending a course of treatment.
Several providers cited system and facility factors as barriers to mutation testing. The most common of these involves the ordering process. Oncology providers often remarked that ordering the mutation test is cumbersome or inconvenient because there is no ordering mechanism in the Computerized Patient Record System (CPRS). Many different approaches for ordering a mutation test exist, including e-mailing the pathology department, calling to place the order, or requesting the test in person. As providers can order many, if not most, other tests via CPRS, it is clear that this presents an inconvenient exception.
Budgetary constraints were another frequently cited system or facility-level barrier. Providers sometimes were unable to access the test due to the cost. Several providers informed the interviewers that the cost of the test is deducted from the pathology department’s budget, and this could present a major constraint to testing. A less commonly cited system or facility level barrier involves the inability to biopsy at the VHA. This was mentioned by only 2 providers who, due to lack of equipment or lack of personnel, were unable to acquire additional tissue samples at their facilities.
Finally, several providers noted that in some cases patients did not wish to undergo a biopsy. Thus, patient preference can act as a barrier to mutation testing. Some patients wish to forgo treatment, which eliminates the need for a mutation test. Other patients believe that due to their smoking history, they are unlikely to have an ALK or EGFR mutation and instead immediately opt for chemotherapy. Only a small minority of participants identified no barriers to mutation testing.
Facilitators for Testing
Many providers complimented the availability of the mutation test. Interestingly, while some providers mentioned that lack of CPRS ordering was a barrier to testing, several also listed access to a CPRS order as a facilitator. These providers commented that ordering a test was streamlined and easy, given the mechanism in CPRS. Some VHA facilities offer CPRS order capabilities, and others do not. Other oncologists commented more generally on the cooperativeness of the pathology department in ordering mutation tests. It seems that facilities may use different ordering procedures, but in most of these facilities, a high degree of cooperation exists between departments to send out for tests that are requested.
Providers offered many ideas for ways to improve mutation testing or to facilitate the testing. By far, the most commonly cited way to improve the testing process was to make mutation testing reflexive for metastatic nonsquamous NSCLC. Some acknowledged that to achieve this would require a change to the budgeting process such that the test would not drain the pathology department’s budget. Implementing reflexive testing of patients, as recommended by guidelines, would understandably address several of the barriers that were identified in this study. Other providers recommended standardizing the ordering procedure and location of results. Specifically, providers recommended creating a button in CPRS for ordering and always reporting the results in the same place in CPRS.
Barriers to GBTT Prescribing
The clear majority of providers identified no barriers to prescribing GBTTs. A few mentioned that they were required to submit a nonformulary consult. A representative quote described this as “more out of a formality, and the pharmacist basically is there with me and he approves it on the spot and provides the prescription on the day, right when I’m seeing the patient.” Only a very small minority of providers identified medication cost as a barrier, but even those respondents did not indicate that cost prevented them from offering GBTTs to their patients. Rather, cost consciousness simply made them more mindful and judicious when making decisions about prescribing GBTTs.