Dr. Wilming is a PGY-1 Pharmacy Practice Resident, Dr. Alford is a General Medicine Clinical Pharmacist, and Dr. Klaus is an Associate Chief of Acute Care Pharmacy and PGY-1 Acute Care Residency Director, all at the VA Portland Health Care System in Oregon. Correspondence: Dr. Wilming (christopher.wilming @va.gov)
Author disclosures The authors report no actual or potential conflicts of interest with regard to this article.
Disclaimer The opinions expressed herein are those of the authors and do not necessarily reflect those of Federal Practitioner, Frontline Medical Communications Inc., the U.S. Government, or any of its agencies. This article may discuss unlabeled or investigational use of certain drugs. Please review the complete prescribing information for specific drugs or drug combinations—including indications, contraindications, warnings, and adverse effects—before administering pharmacologic therapy to patients.
The following QA/QI project was approved locally by the VAPORHCS associate chief of staff/Office of Research and Development and is considered to be nonresearch VHA operations activity and exempt from an institutional review board committee review. This project was a single-center, retrospective chart review of patients admitted to the ICU and general medicine wards at VAPORHCS with acute alcohol withdrawal. The CIWA-Ar protocol order sets between January 1, 2014 and December 31, 2015, were retrieved through the Computerized Patient Record System (CPRS) at VAPORHCS.
Patients with an alcohol withdrawal protocol order set who received gabapentin with or without lorazepam during hospitalization were identified for chart review. Patients were eligible for review if they were aged ≥ 18 years with a primary or secondary diagnosis of acute alcohol withdrawal and had a CIWA-Ar protocol order set placed during hospitalization. Patients must have been administered gabapentin, lorazepam, or both while the CIWA-Ar protocol was active. Patients with an active outpatient prescription for gabapentin or benzodiazepine filled within the previous 30 days, documented history of psychosis or epileptic seizure disorder, or other concomitant benzodiazepines or antiepileptics administered while on the CIWA-Ar protocol were excluded from the analysis.
Baseline characteristics for patients eligible for review were collected and included age; sex; race, body mass index (BMI); estimated creatinine clearance (CrCl); toxicology screen at admission (if available), history of substance use disorder, AWS, or history of withdrawal seizures; and history of a sedative hypnotics (not including benzodiazepines) prescription within 30 days prior to admission.17
The primary endpoint was the total amount of lorazepam administered from the time of admission to the time of discontinuation of the alcohol withdrawal protocol. The dose, frequency, and amount of lorazepam and gabapentin administered daily were collected for each patient while on the CIWA-Ar protocol. Secondary endpoints included rate of the CIWA-Ar score reduction, time to protocol discontinuation, as well as incidence and onset of peak delirium scores during hospitalization. Cumulative CIWA-Ar scores over 24 hours were averaged per patient per day while on CIWA-Ar protocol. Peak CIWA-Ar scores per patient per day on the protocol also were collected. Time to protocol termination was determined by date of order for discontinuation or by date when scoring had ceased and protocol order was inadvertently continued. Peak Intensive Care Delirium Screening Checklist (ICDSC) scores were collected for patients admitted to the ICU.18 Day of peak ICDSC scores also were evaluated.
Statistical Analysis
The sample size for this analysis was determined by the number of patients identified who met the inclusion criteria and did not meet any of the exclusion criteria. Power was not calculated to estimate sample size needed to determine statistical significance. One hundred patients treated for alcohol withdrawal was established as the target sample size for this project. Descriptive statistics were performed to analyze patient baseline characteristics and primary and secondary objective data.
Results
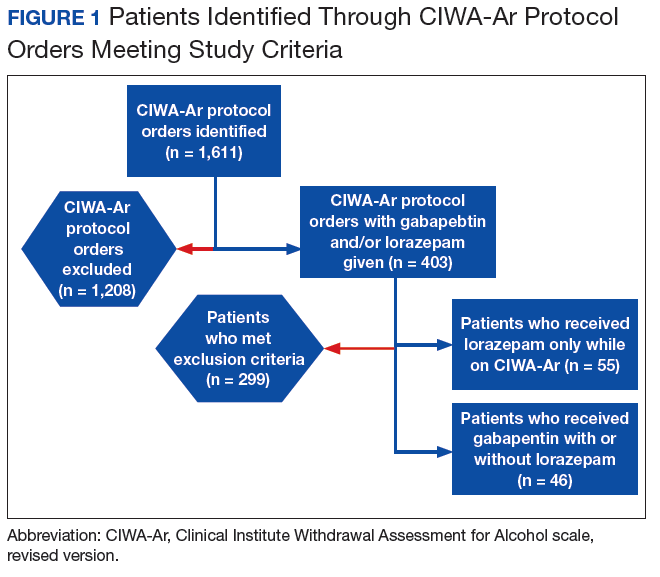
A total of 1,611 CIWA-Ar protocol orders were identified between January 1, 2014 and December 31, 2015.
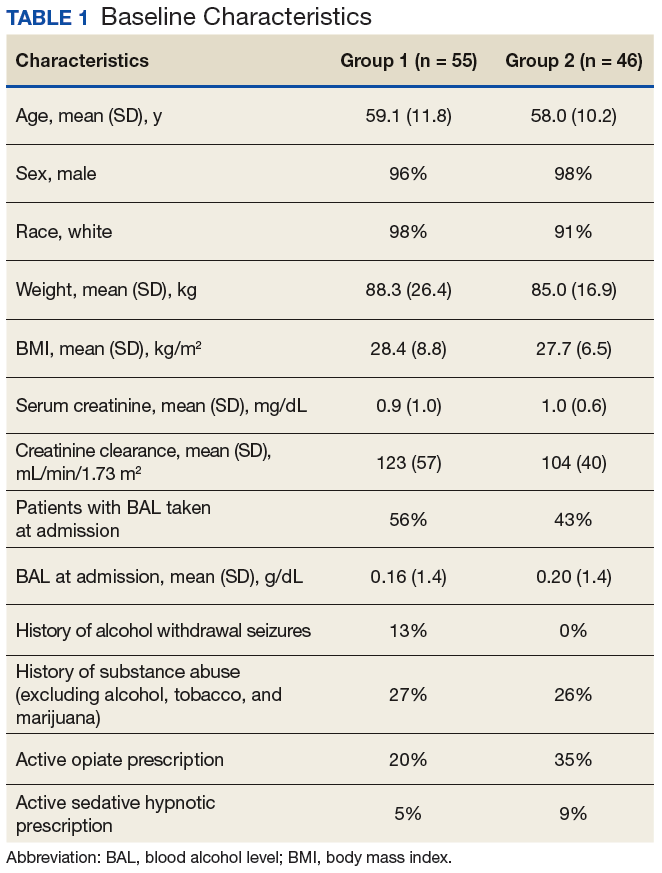
Among these orders, 1,507 met exclusion criteria, leaving 55 patients on CIWA-Ar protocol who received lorazepam only (group 1) and 46 patients who received gabapentin with (n = 36) or without (n = 10) lorazepam (group 2) for alcohol withdrawal management (Figure 1). Baseline characteristics were similar across groups and were characteristic of the patient population treated at VAPORHCS (Table 1),
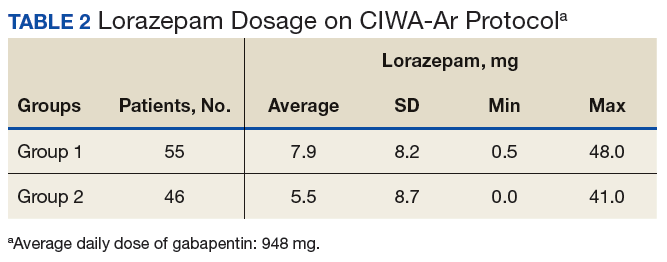
consisting primarily of white males with a mean age of 58 years (± 10) and BMI 28 kg/m2 (± 7). Groups 1 and 2 had similar estimated CrCl at 123 mL/min/1.73 m2 (± 57) and 104 mL/min/1.73 m2 (± 40), respectively. Blood alcohol levels taken at admission were available in 56% and 43% of patients in group 1 and 2 with a mean concentration of 0.16 g/dL (± 1.2) and 0.20 g/dL (± 1.4), respectively. Excluding alcohol, tobacco, and marijuana use, both groups had similar incidence of substance use disorder (26% vs 27%), and 13% of patients in group 1 had a history of alcohol withdrawal seizures vs 0% patients in group 2. Patients who received gabapentin (group 2) from the time of CIWA-Ar protocol initiation until discontinuation received an average daily dose of 948 mg (median 900; min 100/max 3,600, ± 786).
Primary Endpoint
The average amount of lorazepam administered for the total duration on CIWA-Ar protocol was 7.9 mg (median 6, ± 8.2) among
patients in group 1 and 5.5 mg (median 2, ± 8.7) among patients in group 2 (Table 2).
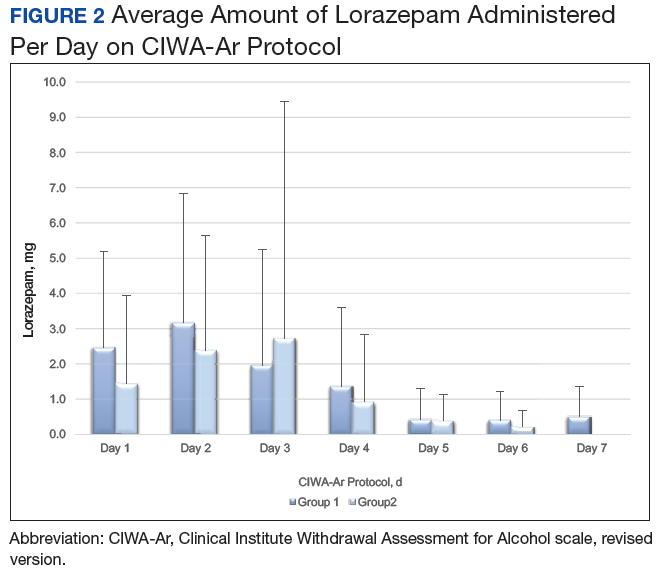
The average amount of lorazepam administered per day on the CIWA-Ar protocol between group 1 and group 2 is shown in Figure 2.