Neha Pathak is a Fee-Basis Staff Physician, and Anne Tomolo is Associate Chief of Staff of Education, both at the Atlanta VA Medical Center in Decatur, Georgia. Cam Escoffery is an Associate Professor in the Department of Behavioral Sciences and Health Education in the Rollins School of Public Health, and Anne Tomolo is an Associate Professor of Medicine in the Division of General Medicine and Geriatrics, both at Emory University in Atlanta. Correspondence: Neha Pathak (nehapathakmd@gmail.com)
Author disclosures The authors report no actual or potential conflicts of interest with regard to this article.
Disclaimer The opinions expressed herein are those of the authors and do not necessarily reflect those of Federal Practitioner, Frontline Medical Communications Inc., the US Government, or any of its agencies.
The original design of the template was informed by the Atlanta PIM team after several informal focus groups and process mapping of CC pathways in the fall of 2015. The participants were all members of the Atlanta PIM team, 2 primary care physicians working with PIM, an AVAMC documentation specialist and a clinical applications coordinator (CAC) assigned to work with PIM. The major themes that arose during the brainstorming discussion were that the template should: (1) be feasible to use during their daily clinic workflow; (2) improve documentation of CC; and (3) have value for spread to other VA sites. Discussion centered on creating a CC Template versatile enough to:
Decrease the number of steps for documenting CC;
Consist only of check boxes, with very little need for free text, with the option to enter narrative free text after template completion;
Document time spent in aggregate for completing complex CC encounters;
Document various types of CC work and modes of communication;
Allow for use by all PIM staff;
Identify all team members that participated in the CC encounter to reduce redundant documentation by multiple staff;
Adapt to different clinic sites based on the varied disciplines participating in other locations;
Use evidence-based checklists to help standardize delivery of CC for certain activities such as TCM; and
Extract data without extensive chart reviews to inform current CC and future QI work.
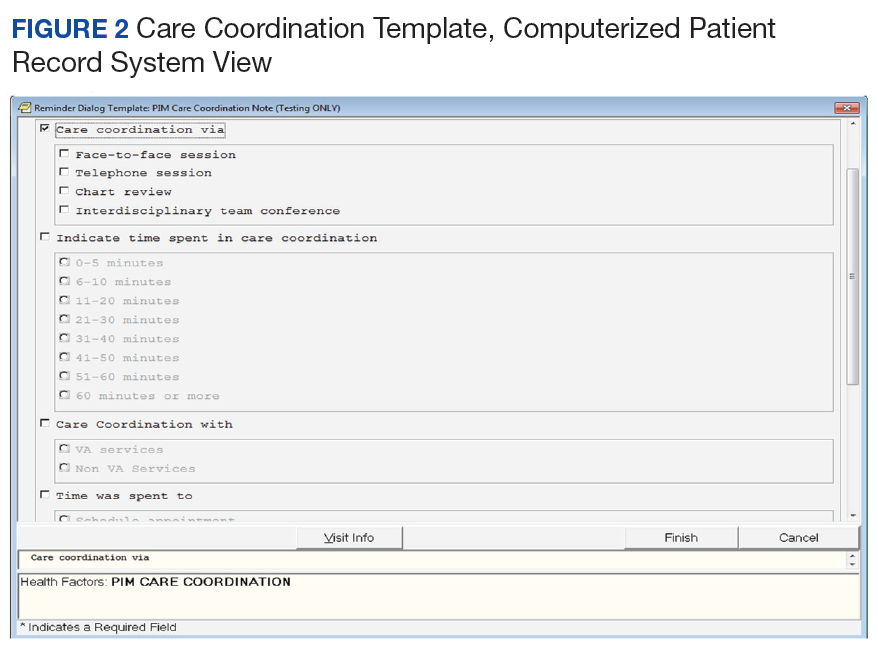
Following the brainstorming sessions, the authors performed a literature review to identify and integrate CC best practices. The AHRQ Care Coordination Atlas served as the main resource in the design of the logic model that depicted the delivery and subsequent documentation of high-quality, evidence-based CC in the CC Template (Figure 2).6
The model offers a framework for evaluation of the implementation process as well as CC outcomes and impacts. The team also adapted discharge strategies from the Re-Engineered Discharge (RED) Toolkit, an evidence-based approach for reducing rehospitalizations, in order to standardize the CC provided and documented by the PIM team during TCM.22
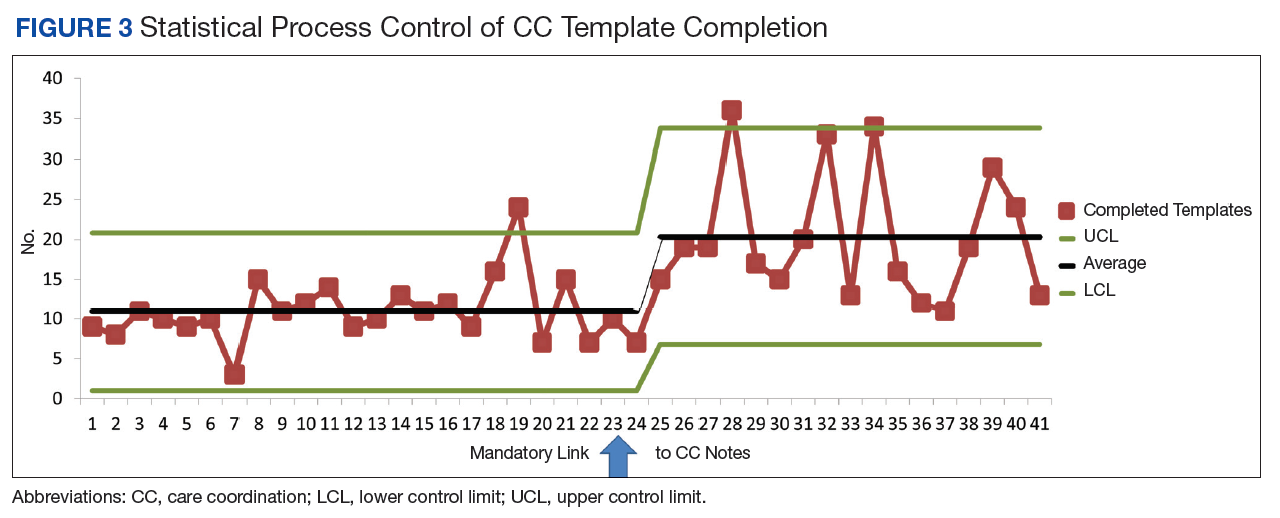
After reaching consensus about the key components of the CC Template, the CAC created a pilot version (Figure 3). All of the elements within the CC Template allowed for data abstraction from the VA Corporate Data Warehouse (CDW) via discrete data elements known as health factors.
The template design allowed PIM team members to document the details of a variety of CC activities, including chart reviews, interdisciplinary team meetings, and multifaceted interventions requiring participation by multiple team members. Figure 1 shows CC Template documentation for the CC examples described. Through an iterative process, the template was redesigned over the pilot period, as selection options were added or removed based on frequency of use.
Over the course of implementation, the team became more enthusiastic about using the CC template to document previously unrecognized CC workload. Because the CC Template only was used to document CC workload and excluded encounters for clinical evaluation and management, specific notes were created and linked with the CC Template for optimal capture of encounters.
All components of the template were mandatory to eliminate the possibility of missing data. The Atlanta PIM site principal investigator developed a multicomponent training designed to increase support for the template by describing its value and to mitigate the potential for variability in how data are captured. Training included a face-to-face session with the team to review the template and work through sample CC cases. Additionally, a training manual with clear operational definitions and examples of how to complete each element of the CC Template was disseminated. The training was subsequently conducted with the San Francisco VA Medical Center PIM team, a spread site, via video conference. The spread site offered significant feedback on clarifying the training documents and adapting the CC template for their distinct care team structure. This feedback was incorporated into the final CC Template design to increase adaptability.