Lisa Glass is a Staff Physician, and Grace Su is Chief of Gastroenterology and Associate Chief of Medicine, both at VA Ann Arbor Healthcare System. Christine Hunt is a Physician Affiliate and Director of the Cooperative Studies Program Epidemiology Centers at Durham VAMC in North Carolina. Michael Fuchs is Chief of Hepatology and Liver Transplantation at Hunter Holmes McGuire VAMC. Christine Hunt is an Adjunct Associate Professor of Medicine at Duke University Medical Center in Durham. Lisa Glass is an Assistant Professor and Grace Su is a Professor of Medicine, both at the University of Michigan Medical School in Ann Arbor. Michael Fuchs is Professor of Medicine at Virginia Commonwealth University in Richmond. Correspondence: Lisa Glass (lisaglas@med.umich.edu)
Author disclosures The authors report no actual or potential conflicts of interest with regard to this article.
Disclaimer The opinions expressed herein are those of the authors and do not necessarily reflect those of Federal Practitioner, Frontline Medical Communications Inc., the US Government, or any of its agencies. This article may discuss unlabeled or investigational use of certain drugs. Please review the complete prescribing information for specific drugs or drug combinations—including indications, contraindications, warnings, and adverse effects—before administering pharmacologic therapy to patients.
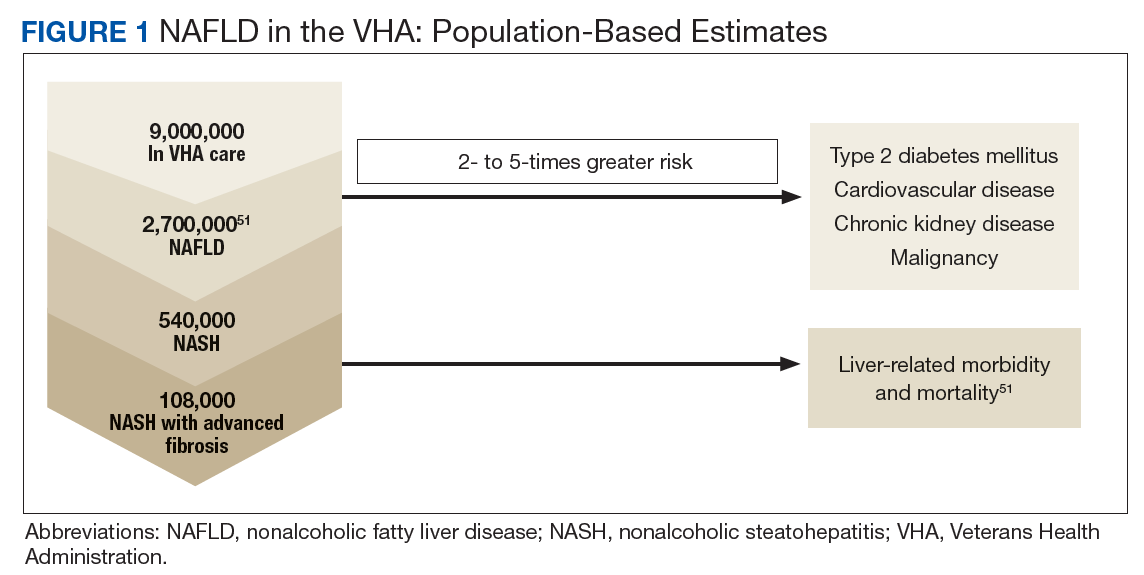
Nonalcoholic fatty liver disease (NALFD) is now the most common chronic liver disease in the developed world and affects about 25% to 30% of adults in the US and 30% of veterans who receive care in the VHA system (Figure 1).
Comprised of a spectrum of disease severity, NAFLD ranges from simple steatosis to nonalcoholic steatohepatitis ([NASH] steatosis with hepatocyte inflammation, necrosis, and fibrosis). Patients with NALFD have significantly increased mortality because of both hepatic (such as cirrhosis and hepatocellular carcinoma [HCC]) and extrahepatic complications (such as metabolic syndrome [MetS], cardiovascular disease [CVD], and malignancy). In this article, we will focus on the extrahepatic manifestations of NAFLD and its impact on diagnosis and management.
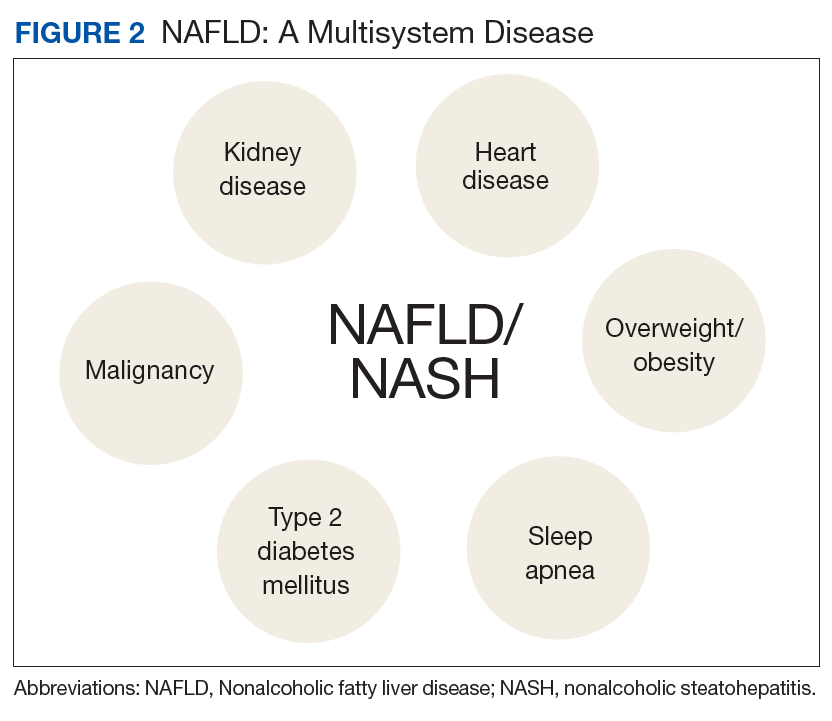
NAFLD is significantly associated with the presence of MetS, so much so that it has been considered the hepatic manifestation of MetS. NAFLD also is strongly associated with type 2 diabetes mellitus (T2DM), CVD, chronic kidney disease (CKD), and obstructive sleep apnea (OSA) (Figure 2).
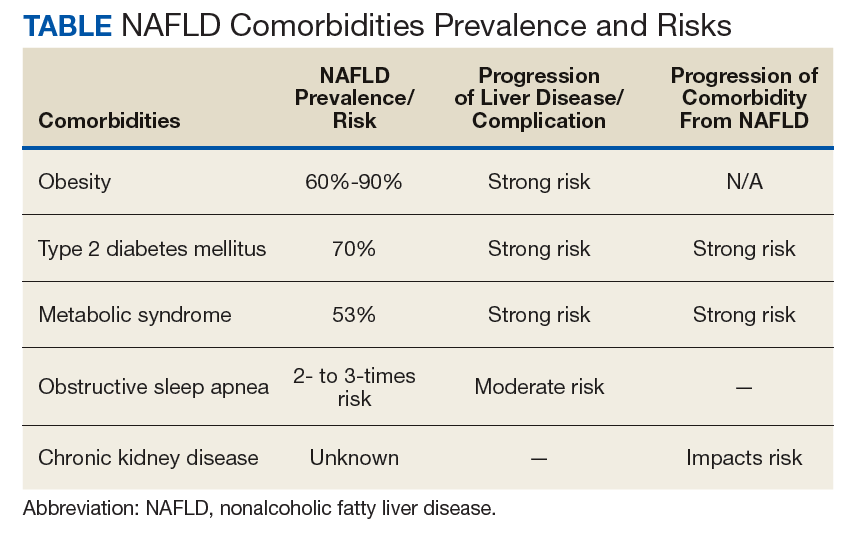
Although these associations may result from shared risk factors, strong evidence suggests that for some of the factors at least, there is bidirectional influence on the natural history of the other comorbid conditions (Table).
This means that the management of NAFLD can help improve the management of comorbidities and vice versa. This is important, as the primary cause of mortality in patients with NAFLD, particularly in those without advanced fibrosis or cirrhosis,is related to CVD and extrahepatic malignancy and not from liver disease.
Obesity/Visceral Adiposity
Obesity (body mass index [BMI] > 30) prevalence in the US has almost doubled over the past 30 years and continues to climb.1 Obesity affects 41% of veterans in the Veterans Health Administration and is the most common risk factor for NAFLD.2 NAFLD is 4 times more prevalent in obese patients, thus, it is not surprising that 80% to 90% of patients evaluated in bariatric centers have NAFLD, reported in 2 large series.3,4 Increased BMI and waist circumference predict the presence of NASH and advanced fibrosis.5
While obesity is a hallmark for NAFLD, particularly in the US, it is important to note that up to 20% of Americans with normal BMI have NAFLD, based on findings of steatosis on ultrasound.6 These patients with lean NAFLD are often underdiagnosed. In addition to the patient’s BMI, it is important to recognize that in NAFLD, the distribution and type of fat deposition is more important than just BMI. Visceral fat refers to fat accumulation within the abdominal cavity and is key to the pathogenesis of NAFLD. Visceral fat, compared with subcutaneous fat, is metabolically active and can deliver an overabundance of free fatty acids to the liver as well as secrete proinflammatory mediators in the setting of insulin resistance. Visceral fat stores can predict increased hepatic fat content, inflammation, and fibrosis.5 Thus, it is important to recognize that those patients with relatively more visceral fat are more prone to NAFLD. The best clinical indicator of visceral adiposity is abdominal obesity, indicated by waist circumference > 40 inches in men and > 35 inches in women.