Camilla Pimentel is a Research Health Scientist at the Center for Healthcare Organization and Implementation Research and the New England Geriatric Research Education and Clinical Center (GRECC), and Megan Gately is a Program Manager and Lauren Moo is Site Director at the New England GRECC, Edith Nourse Rogers Memorial Veterans Hospital in Bedford, Massachusetts. Steven Barczi is a Physician at Madison GRECC, William S. Middleton Memorial Veterans Hospital in Wisconsin. Kenneth Boockvar is Associate Director (research), Judith Howe is Deputy Director, and William Hung is Associate Director (clinical) at Bronx/NY Harbor GRECC, James J. Peters Veterans Affairs Medical Center in New York. Ella Bowman is a Geriatrician and Alayne Markland is Associate Director (clinical) at the Birmingham/Atlanta GRECC in Alabama. Thomas Caprio is a Geriatrician at the Canandaigua VA Medical Center in New York. Cathleen Colón-Emeric is Associate Director (clinical) at the Durham GRECC, Durham VA Medical Center in North Carolina. Stuti Dang and Willy Valencia-Rodrigo are Geriatricians at the Miami GRECC, Miami VA Healthcare System in Florida. Sara Espinoza is Associate Director (clinical) at the San Antonio GRECC, Audie L. Murphy Memorial VA Hospital in Texas. Kimberly Garner is Associate Director (education & evaluation) at the Little Rock GRECC, Central Arkansas Veterans Healthcare System. Patricia Griffiths is a Research Health Scientist at the Birmingham/ Atlanta GRECC, Atlanta VA Medical Center in Decatur, Georgia. Hillary Lum is a Geriatrician at the Eastern Colorado GRECC, VA Eastern Colorado Health Care System in Denver. Michelle Rossi is Associate Director (clinical) at the Pittsburgh GRECC, VA Pittsburgh Healthcare System in Pennsylvania. Stephen Thielke is Associate Director (education & evaluation) at the Puget Sound GRECC, Puget Sound VA Medical Center in Seattle, Washington.
Author affiliations can be found at the end of the article. *Both authors contributed equally to this manuscript. Correspondence: Camilla Pimentel (Camilla.Pimentel@va.gov)
Author disclosures The authors report no actual or potential conflicts of interest with regard to the article.
Disclaimer The opinions expressed herein are those of the authors and do not necessarily reflect those of Federal Practitioner, Frontline Medical Communications Inc., the U.S. Government, or any of its agencies.
GRECC Connect was established under the umbrella of the VA Geriatric Scholars Program, which since 2008 integrates geriatrics into rural primary care practices through tailored education for continuing professional development.11 Through intensive courses in geriatrics and quality improvement methods and through participation in local quality improvement projects benefiting older veterans, the Geriatric Scholars Program trains rural PCPs so that they can more effectively and independently diagnose and manage common geriatric syndromes.12 The network of clinician scholars developed by the Geriatric Scholars Program, all rural frontline clinicians at VA clinics, has given the GRECC Connect project a well-prepared, geriatrics-trained workforce to act as project champions at rural CBOCs and VAMCs. The GRECC Connect project’s goals are to enhance access to geriatric specialty care among older veterans with complex medical problems, geriatric syndromes, and increased risk for institutionalization, and to provide geriatrics-focused educational support to rural HCP teams.
Geriatric Provider Consultations
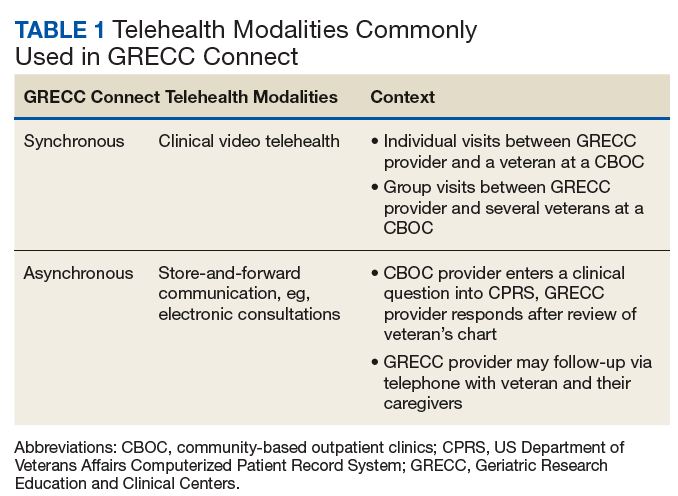
The first overarching goal of the GRECC Connect project is to improve access to geriatrics specialty care by facilitating linkages between GRECC hub sites and the CBOCs and VAMCs that primarily serve veterans in rural communities. GRECC hub sites offer consultative support from geriatrics specialty team members (eg, geriatricians, nurse practitioners, pharmacists, gero- or neuropsychologists, registered nurses [RNs], and social workers) to rural PCP in their catchment area. This support is offered through a variety of telehealth modalities readily available in the VA (Table 1). These include CVT, in which a veteran located at a rural CBOC is seen using videoconferencing software by a geriatrics specialty provider who is located at a GRECC hub site. At some GRECC hub sites, CVT has also been used to conduct group visits between a GRECC provider at the hub site and several veterans who participate from a rural CBOC. Electronic consultations, or e-consults, involve a rural provider entering a clinical question in the VA Computerized Patient Record System. The question is then triaged, and a geriatrics provider at a GRECC responds, based on review of that veteran’s chart. At some GRECC hub sites, the e-consults are more extensive and may include telephone contact with the veteran or their caregiver.
Consultations between GRECC-based teams and rural PCPs may cover any aspect of geriatrics care, ranging from broad concerns to subspecialty areas of geriatric medicine. For instance, general geriatrics consultation may address polypharmacy, during either care transitions or ongoing care. Consultation may also reflect the specific focus area of a particular GRECC, such as cognitive assessment (eg, Pittsburgh GRECC), management of osteoporosis to address falls (eg, Durham GRECC, Miami GRECC), and continence care (eg, Birmingham/Atlanta GRECC).13 Most consultations are initiated by a remote HCP who is seeking geriatrics expertise from the GRECC team.
Some GRECC hub sites, however, employ case finding strategies, or detailed chart reviews, in order to identify older veterans who may benefit from geriatrics consultation. For veterans identified through those mechanisms, the GRECC clinicians suggest that the rural HCP either request or allow an e-consult or evaluation via CVT for those veterans. The geriatric consultations may help identify additional care needs for older veterans and lead to recommendations, orders, or remote provision of a variety of other actions, including VA or non-VA services (eg, home-based primary care, home nursing service, respite service, social support services such as Meals on Wheels); neuropsychological testing; physical or occupational therapy; audiology or optometry referral; falls and fracture risk assessment and interventions to reduce falls (eg, home safety evaluation, physical therapy); osteoporosis risk assessments (eg, densitometry, recommendations for pharmacologic therapy) to reduce the risk of injury or nontraumatic fractures from falls; palliative care for incontinence and hospice; and counseling on geriatric issues such as dementia caregiving, advanced directives, and driving cessation.
More recently, the Miami GRECC has begun evaluating rural veterans at risk for hypoglycemia, providing patient education and counseling about hypoglycemia, and making recommendations to the veterans’ primary care teams.14 Consultations may also lead to the appropriate use or discontinuation of medications, related to polypharmacy. GRECC-based teams, for example, have helped rural HCPs modify medication doses, start appropriate medications for dementia and depression, and identify and stop potentially inappropriate medications (eg, those that increase fall risk or that have significant anticholinergic properties).15