News

Having unmet social needs ups cardiovascular risk
WASHINGTON – Food and transportation for patients need to be addressed to help patients decrease their cardiovascular risks.
Introduction: Recently, numerous studies have linked social determinants of health (SDoH) with clinical outcomes. While this association is well known, the interfacility variability of these risk favors within the Veterans Health Administration (VHA) is not known. Such information could be useful to the VHA for resource and funding allocation. The aim of this study is to explore the interfacility variability of 5 SDoH within the VHA.
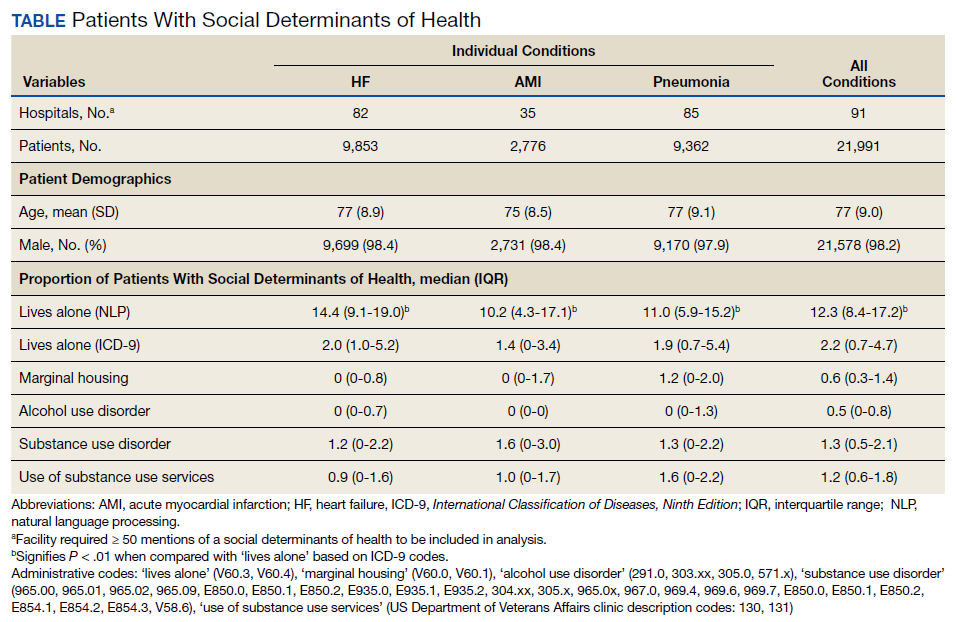
Methods: In a cohort of patients (aged ≥ 65 years) hospitalized at VHA acute care facilities with either acute myocardial infarction (AMI), heart failure (HF), or pneumonia in 2012, we assessed (1) the proportion of patients with any of the following five documented SDoH: lives alone, marginal housing, alcohol use disorder, substance use disorder, and use of substance use services, using administrative diagnosis codes and clinic stop codes; and (2) the documented facility-level variability of these SDoH. To examine whether variability was due to regional coding differences, we assessed the variation of living alone using a validated natural language processing (NLP) algorithm.
Results: The proportion of veterans admitted for AMI, HF, and pneumonia with SDoH was low. Across all 3 conditions, lives alone was the most common SDoH (2.2% [interquartile range (IQR), 0.7-4.7]), followed by substance use disorder (1.3% [IQR, 0.5-2.1]), and use of substance use services (1.2% [IQR, 0.6-1.8]). Using NLP, the proportion of hospitalized veterans with lives alone was higher for HF (14.4% vs 2.0%, P < .01), pneumonia (11% vs 1.9%, P < .01), and AMI (10.2% vs 1.4%, P < .01) compared with International Classification of Diseases, Ninth Edition codes. Interfacility variability was noted with both administrative and NLP extraction methods.
Conclusions: The presence of SDoH in administrative data among patients hospitalized for common medical issues is low and variable across VHA facilities. Significant facility-level variation of 5 SDoH was present regardless of extraction method.
WASHINGTON – Food and transportation for patients need to be addressed to help patients decrease their cardiovascular risks.
A novel health education and implementation group for older veterans targeted behaviors known to support cognitive functioning.
The Heart Disease Reversal Program is a streamlined adaptation of behavioral/lifestyle interventions aimed at promoting partial reversal of...