Jasmine Carpenter is a Mental Health Clinical Pharmacy Specialist; Tiffany Lee is a Geriatric Clinical Pharmacy Specialist; and Elizabeth Green is a Women’s Clinic Psychiatrist; all at the Washington Veterans Affairs Medical Center in the District of Columbia. Eileen Holovac is an Oncology Clinical Pharmacy Specialist at the Palo Alto Veterans Affairs Medical Center in California. Correspondence: Jasmine Carpenter (jasmine.carpenter@va.gov)
Author disclosures The authors report no actual or potential conflicts of interest with regard to this article.
Disclaimer The opinions expressed herein are those of the authors and do not necessarily reflect those of Federal Practitioner, Frontline Medical Communications Inc., the US Government, or any of its agencies. This article may discuss unlabeled or investigational use of certain drugs. Please review the complete prescribing information for specific drugs or drug combinations—including indications, contraindications, warnings, and adverse effects—before administering pharmacologic therapy to patients.
Background: Suicide is a global phenomenon and is the 10th leading cause of death in the US. Veterans are more likely to die by suicide than those in the general population. In 2018, the suicide rate for all US veterans was 1.5 times higher than the rate for nonveterans, after adjusting for population differences in age and sex. In light of this disparity, suicide prevention is one of the highest priorities for the US Department of Veterans Affairs (VA). One major goal of the VA suicide prevention strategy is to reduce access to lethal means.
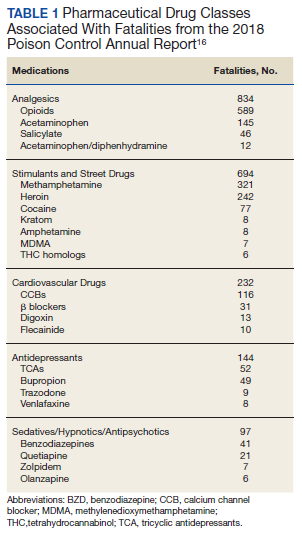
Observations: This article will provide information on medications with high lethality and a stepwise approach for how health care providers may limit lethal medications for patients at high risk for suicide. The first step is to determine suicide risk. More than 90% of those who die by suicide have a psychiatric diagnosis at the time of death. Clinicians can use risk assessment tools, such as the Veterans Health Administration Suicide Prevention Population Risk Identification and Tracking for Exigencies tool. The second step is to identify substances strongly associated with fatalities. According to the American Association of Poison Control Centers, the pharmaceutical classes associated with the largest number of fatalities are stimulants and street drugs, followed by analgesics, cardiovascular agents, antidepressants, antipsychotics, and sedatives/hypnotics. The third step is to consider potential drug-drug interactions, such as the combination of opioids and sedative-hypnotics. Finally, clinicians need to address risks. With high-risk patients it may be preferential to prescribe medications that are less lethal. All patients with a high risk of suicide should receive lethal means counseling.
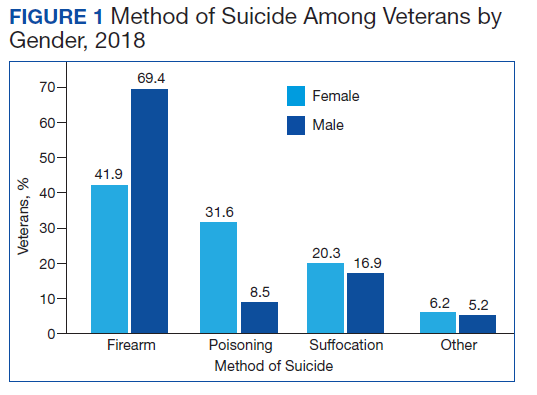
Conclusions: While firearms continue to be the most lethal means for veteran suicide, intentional poisoning with medications or substances also is a common method for suicide, especially for female veterans. Having knowledge of medications with high lethality and limiting access to these agents can be a successful strategy for reducing suicide deaths.
Suicide is a global phenomenon and a worldwide public health concern.1 The World Health Organization estimates that > 800,000 people die by suicide every year. In the US, suicide is the 10th leading cause of death, and on average, 129 Americans die by suicide each day.2 In 2018, the suicide rate for all veterans was 1.5 times higher than the rate for nonveterans, after adjusting for population differences in age and sex. Among female veterans, the rate of suicide was 2.1 times higher than the rate for female nonveterans.3
In light of this disparity, suicide prevention is one of the highest priorities for the US Department of Veterans Affairs (VA). In 2018, the VA developed and published the National Strategy for Preventing Veteran Suicide.4 One major goal of this strategy is to reduce access to lethal means (ie, firearms, medications, chemicals, or poisons) among veterans at high risk for suicide. Reducing access to lethal means has been found to decrease suicide rates.4,5
Drug overdose is a leading method for suicide attempts, especially for female veterans.3,6 Although the overall case fatality ratio for overdose is < 2%, drug overdose accounted for 59.4% of suicide attempts and 13.5% of deaths by suicide from 2007 to 2014.6,7 Within the veteran population, the majority of suicide deaths in 2018 were due to self-inflicted firearm injury for both male and female veterans, followed by poisoning via substances and pharmaceutical agents for female veterans (Figure 1).3 Notably, when compared with men, women were more likely to choose drug overdose as a method for suicide. One study found that women aged < 45 years used drug and poison ingestion in 9 out of 10 suicide attempts.6 Since some medications are more lethal than others, interventions to limit the availability of lethal medications may prevent deaths and reduce the severity of suicide attempts. This article will provide a stepwise approach to help clinicians identify and limit lethal medications for patients at high risk for suicide.
Step 1: Determine Suicide Risk
Although it is impossible to predict with certainty an individual’s risk of suicide, several patient characteristics and life circumstances have been identified as risk factors. The strongest predictor of suicide is the presence of psychiatric disease.8 More than 90% of those who have had a death by suicide have a psychiatric diagnosis at the time of death, and suicide rates in those with mental illness are at least 10 times as high as in the general population.9,10 Depression is the leading cause of death by suicide worldwide, followed by substance-related disorders (22.4%), personality disorders (11.6%), schizophrenia (10.6%), and anxiety/somatoform disorders (6.1%).8,11-13
Clinicians also can use various risk assessment tools to identify patients at high risk for suicide. The Veterans Health Administration (VHA) Stratification Tool for Opioid Risk Mitigation (STORM) calculates patients’ risk based on data extracted from the electronic health record and is less time intensive, more easily refined, and may be more powerful than standard risk assessment tools because it can be deployed on a large scale.14,15 The VHA also developed the Suicide Prevention Population Risk Identification and Tracking for Exigencies (SPPRITE) tool to assist clinicians in tracking patients with current (or recent) high levels of suicide risk. This tool unifies specific patient information gathered from the patient’s electronic health record and from other predictive model dashboards (such as STORM).
Step 2: Identify Substances Strongly Associated With Fatalities
According to the American Association of Poison Control Centers (AAPCC), the pharmaceutical classes associated with the largest number of fatalities are analgesics, followed by stimulants and street drugs, cardiovascular agents, antidepressants, antipsychotics, and sedatives/hypnotics (Table 1).16 Stimulants and street drugs accounted for 694 fatalities of 39,238 single-substance exposures (mortality rate: 1.8%).16 Drugs of abuse, including cocaine, hallucinogenic amphetamines, heroin, and kratom, have shown an increased trend in use.16