Leah Nguyen is an Emergency Medicine Clinical Pharmacy Specialist at the Portland Veterans Affairs Health Care System in Oregon; Andrew Varker is an Infectious Disease Clinical Pharmacy Specialist; Pamela Slaughter and Daniel Boyle are Emergency Medicine Clinical Pharmacy Specialists; Negin Nekahi is an Infectious Disease Specialist; Leah Nguyen was a Pharmacy Resident at the time this article was written; all at Phoenix Veterans Affairs Health Care System in Arizona. Correspondence: Leah Nguyen (leah.nguyen1@va.gov)
Author disclosures
The authors report no actual or potential conflicts of interest with regard to this article.
Disclaimer
The opinions expressed herein are those of the authors and do not necessarily reflect those of Federal Practitioner, Frontline Medical Communications Inc., the US Government, or any of its agencies. This article may discuss unlabeled or investigational use of certain drugs. Please review the complete prescribing information for specific drugs or drug combinations—including indications, contraindications, warnings, and adverse effects—before administering pharmacologic therapy to patients.
Purpose: Acute exacerbations of chronic obstructive pulmonary disease (AECOPD) can be caused by viral, bacterial, or environmental factors. Recent studies have suggested that procalcitonin serum levels may help reduce unnecessary antibiotic use without statistically significant differences in rates of treatment failure for AECOPD. The purpose of this quality improvement project was to create a procalcitonin-based algorithm to aid emergency department (ED) clinicians in the management of patients with AECOPD who do not require hospitalization and to evaluate its efficacy and practicality. The primary outcome of this project was the rate of antibiotic prescriptions before and after the initiation of the algorithm.
Methods: This study used an observational, retrospective, pre- and posteducation/intervention design. Clinicians were educated individually on the use of procalcitonin, and a copy of the algorithm was made available to each clinician and posted in the ED. Patients who were discharged from the ED with a diagnosis of an AECOPD were identified using International Classification of Diseases , Tenth Revision codes. Patient charts were reviewed from November 2018 to March 2019 for the preimplementation period and November 2019 to March 2020 for the postimplementation period. The rate of antibiotic prescriptions and the number of procalcitonin tests ordered before and after the introduction of the algorithm were analyzed. In addition, information on COPD Global Initiative for Chronic Obstructive Lung Disease (GOLD) grouping and 30-, 60-, and 90-day reexacerbation rates were collected. It was estimated that a sample size of 146 patients (73 patients/group) would provide 80% power to detect a between-group difference of 10% in the percentage of patients who were prescribed antibiotics. Categorical variables were expressed using estimates of their frequency and percentages. Percentages were compared using Fisher exact tests. For all tests, the significance level was set at 0.05.
Results: Seventy-three patients were included in the preintervention group, and 77 patients were included in the postintervention group. Patients in the preintervention and postintervention groups had similar representation in GOLD categories: 52% and 51% for D, 17.8% and 23.4% for C, 21.9% and 16.8% for B, and 8.2% and 7.8% for A, respectively. The rate of antibiotic prescriptions decreased by 20% after implementation from 83.6% before to 63.6% after implementation ( P = .01). The differences in reexacerbation rates between the preintervention and postintervention groups were similar: 19.2% vs 23.4% at 30 days, 12.3% vs 11.7% at 60 days, and 4.1% vs 9.1% at 90 days, respectively. Prior to education and introduction of the procalcitonin algorithm, procalcitonin was ordered for 1.4% of AECOPD cases. Postimplementation, procalcitonin was ordered for 28.6% of AECOPD cases and used in clinical decision making 81.8% of the time .
Conclusions: In this study of the implementation of a treatment algorithm for patients with mild and moderate AECOPD who present to the ED, procalcitonin was shown to reduce the rate of antibiotic prescriptions without an observable difference in reexacerbation rates 30, 60, and 90 days after presentation.
The Global Initiative for Chronic Obstructive Lung Disease (GOLD) guidelines define acute exacerbations of chronic obstructive pulmonary disease (AECOPD) as a sudden worsening of respiratory symptoms that require additional interventions. Exacerbations are classified as mild (treated with short-acting bronchodilators only), moderate (treated with antibiotics and/or oral corticosteroids), or severe (treatment requiring hospitalization). Exacerbations must include increased dyspnea, and other symptoms may involve increased sputum volume and purulence, cough, and a change in sputum color. These symptoms can be due to viral, bacterial, or environmental causes, with viral respiratory infections being the most common cause.1-4 However, determining the etiology of an exacerbation can be difficult based on symptoms alone and can lead to an excessive and unnecessary use of antibiotics. Only the change in sputum color is considered highly sensitive and specific for bacterial causes.1 As a result, there has been an increased interest in the use of acute biomarkers to determine whether antibiotics are necessary.
Procalcitonin (PCT) is an acute phase reactant that increases in response to inflammation, especially inflammation caused by a bacterial infection. Recent studies have suggested that PCT may be used in patients experiencing an AECOPD to reduce antibiotic use without impacting rates of treatment failure.5-9 A majority of these studies have been in the inpatient setting or a combination of inpatient and outpatient settings.
The purpose of this study was to create and to evaluate the efficacy and practicality of a PCT-based algorithm to aid emergency department (ED) clinicians in the evaluation of patients with AECOPD who do not require hospitalization. The primary outcome of this project was the rate of antibiotic prescriptions before and after the initiation of the algorithm.
Methods
This was an observational, retrospective, pre/post assessment at the Phoenix Veterans Affairs Health Care System (PVAHCS) in Arizona. Patients who were discharged from the ED with a diagnosis of an AECOPD were identified using International Classification of Diseases, Tenth Revision (ICD-10) codes. Patient charts were reviewed from November 2018 to March 2019 for the preimplementation group and from November 2019 for March 2020 in the postimplementation group. The periods were chosen to reflect similar seasons for both the pre- and postimplementation interventions. Patients were excluded from analysis if they required hospital admission, were immunocompromised, on chronic antimicrobial therapy, had no documented medical history of COPD, or if they were presenting primarily for medication refills. Information collected included the rate of antibiotic prescriptions, procalcitonin test orders, COPD GOLD classification, and 30-, 60-, and 90-day reexacerbation rates.
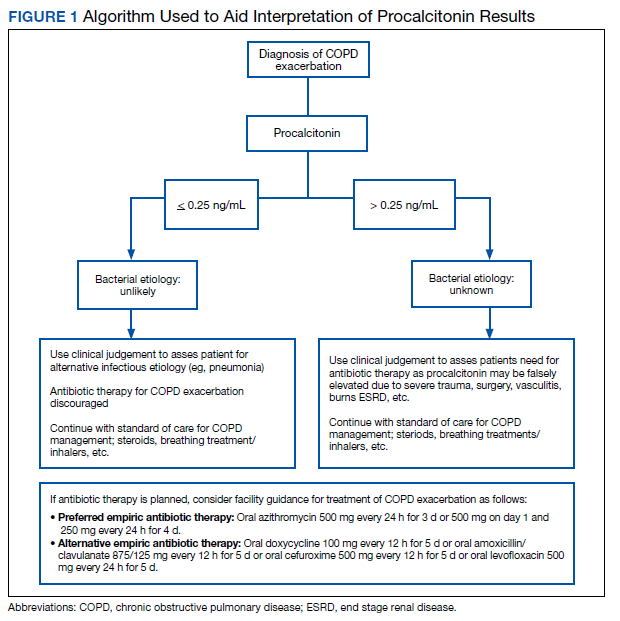
A PCT-based algorithm (Figure 1) was developed and approved by the PVAHCS Antimicrobial Stewardship Program, the Pharmacy and Therapeutics committee, and ED leadership. PCT threshold values were based on values approved by the US Food and Drug Administration and previous studies—antibiotics were discouraged for PCT levels ≤ 0.25 ng/mL but could be considered for PCT levels > 0.25 ng/mL.5,8,9 Clinicians were not required to use the algorithm, and the use of clinical judgement was encouraged. The recommended antibiotic therapies were based on previously approved PVAHCS antimicrobial stewardship guidance. To promote utilization, a PCT quick order option was added to the ED laboratory order menu.
ED clinicians were individually educated by the antimicrobial stewardship and emergency medicine pharmacists, an infectious disease physician champion, and the pharmacy resident. Clinicians were educated about PCT and its use in the setting of AECOPD to aid in the determination of bacterial infections. Each clinician received an electronic copy the algorithm and summary of the study protocol before implementation and 3 months after implementation for follow-up education. In addition, a printed copy of the algorithm was posted in multiple clinician workstations within the ED. For the first month of implementation, the project lead was available full-time in the ED to encourage algorithm use and to field questions or concerns from clinicians.
Outcome Measures
The primary outcome was the rate of antibiotic prescriptions pre- and postintervention. The safety endpoints were 30-, 60-, and 90-day reexacerbation rates. Reexacerbation rates were defined by ICD-10 codes and documentation from a primary care visit or subsequent ED visit. The secondary outcomes were the rate of PCT tests ordered and used for treatment decisions. Other areas of interest were antibiotic prescribing trends, duration of therapy, and patient COPD GOLD classification.
Statistical analysis
It was estimated that a sample size of 146 patients (73 patients/group) would provide 80% power to detect a between-group difference of 10% in the percentage of patients who were prescribed antibiotics. Categorical variables were expressed using estimates of frequency and percentages. Percentages were compared using Fisher exact tests. For all tests, the significance level was set at 0.05.