Local vs Federal Policy
By 2009, 15 states had passed legislation allowing the medical use of marijuana. Many VA hospitals and clinics continued to regard marijuana, whether prescribed or not, as an illicit drug that violated opioid contracts or agreements. The clinical justification for these denials or other treatment plan modifications was to ensure that veterans used marijuana safely, for example, through detecting and preventing drug interactions or impairment of driving ability.
A group called Veterans for Medical Marijuana Access, founded by veteran Michael Krawitz, was the most politically active among veterans’ organizations on the issue of medical marijuana. Astutely, Mr. Krawitz and other advocates did not aim to change federal law and the Supremacy Clause or the court’s interpretations of the Commerce Clause as it applied to medical marijuana. Instead, their strategy was to expand veterans’ access to state programs, and their tactic was to work directly with the VA to formulate a policy. Mr. Krawitz adroitly used the media to champion his cause.
On March 5, 2010, Krawitz received a letter from Col. Will A. Gunn of the VA OGC. Mr. Krawitz had written the VA OGC regarding the inequities in VA policy regarding the provision of opioid medications for pain management to veterans enrolled in state medical marijuana programs. Mr. Krawitz informed Col. Gunn that the directors of some facilities had issued policies explicitly stating that veterans who provide medical marijuana registration in accordance with state programs and who tested positive for the drug would not be considered in violation of opioid contracts. Mr. Krawitz asked for official confirmation that these local policies were valid. On July 6, 2010, Under Secretary for Health Dr. Robert Petzel wrote Mr. Krawitz a memorandum stating, “If a veteran obtains and uses medical marijuana in a manner consistent with state law, testing positive for marijuana would not preclude the veteran from receiving opioids for pain management in a Department of Veterans Affairs facility.”
Dr. Petzel also outlined what would become the clinical ethics principles VA would employ to manage the federal-state law conflict regarding medical marijuana. First, a patient must inform his provider of medical marijuana use to ensure safety. Second, opioid agreements must make a clear distinction between illegal drugs, including the recreational use of marijuana, and medical marijuana. Third, the practitioner has the discretion to make the opioid prescribing decision and must make that decision on clinical grounds. Fourth, the prescribing decision should be made on a case-by-case basis “based upon the provider’s judgment and the needs of the patient.”
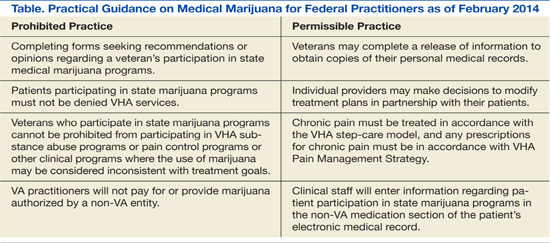
Following these letters was a highly publicized article in The New York Times in which Principal Deputy Under Secretary for Health Dr. Robert L. Jesse confirmed the new policy.15 The article included comments from Mr. Krawitz on the change in VA’s approach to medical marijuana. The VHA codified these less formal communications in VHA Directive 2010-035 issued on July 22, 2010.16 This directive was rescinded and replaced in January 2011 by VHA Directive 2011-004, which remains in effect as of this article’s publication.17 The provisions of this directive titled “Access to Clinical Programs for Veterans Participating in State-Approved Medical Marijuana Programs” are summarized in the Table as practical guidance for federal practitioners.
In contrast to the VA, the DoD has not revised its position that the use and possession of marijuana for any purpose is a violation of the Uniform Code of Military Justice.18 There is no indication that the DoD plans to change its ruling that military personnel who use or possess marijuana are subject to court martial, even in states where marijuana is available for therapeutic purposes.
Clinical Considerations
Concerns and questions from practitioners in the field about how to practically implement the opinion of VA OGC and VHA Directive 2010-035 led the Office of Patient Care Services (PCS) in August 2010 to issue clinical guidance that has significant ethical implications.2
Veterans who are certified to use medical marijuana should present evidence of their registration, often a medical marijuana card, to their VA provider. The provider is then advised to ask the patient to sign a release of information to enable the VA practitioner to speak to the non-VA counterpart who is prescribing the medical marijuana. This approach respects the patient’s confidentiality and obtains informed consent for coordinated treatment. One limitation of this guidance is that it does not advise the practitioner how to proceed if the patient refuses to sign the release. The VA confidentiality regulations regarding substance use information are the strictest of all federal privacy laws. Under 38 USC 7332, this information cannot be released without the explicit written consent of the veteran in order to prevent stigma and discrimination.19 The ethical objective of this communication between VA and community practitioners is nonmaleficence and thus is focused on “adherence monitoring, treatment effectiveness, safety, and impact on cognitive, emotional, social and physical functioning, and side-effects.”20