A facilitator manages each simulation, based on a scripted scenario or teaching film viewed by workshop participants. In the simulations attendees assume the roles of hospital staff that might be realistically involved in disclosure conversations, including executive leaders, physicians, nurses, risk managers, pharmacists, chaplains, and social workers.
Simulations average 5 to 7 minutes and are followed by a debriefing, including simulation participants, workshop facilitators, and the professional actor, who remain in character. By the end of each 2-day workshop, all attendees have participated in multiple small-group simulations of both clinical and institutional disclosures. Pre- and postworkshop knowledge questions and program evaluation data are collected with immediate-response polling technology used throughout the workshop.
Between 20 and 40 HCPs attended each workshop, which was designed for clinical and administrative leaders as well as others supporting the disclosure process, such as nurse managers, patient safety managers, social workers, chaplains, and pharmacists. The facility director, chief of staff, risk manager, and lawyers from the Regional Counsel office all play an important role in institutional disclosures and all were strongly encouraged to attend. The DTP facilitators observed the importance of senior executive leadership—participation, which enhanced dialogue in the large group sessions and small-group simulation-based learning.
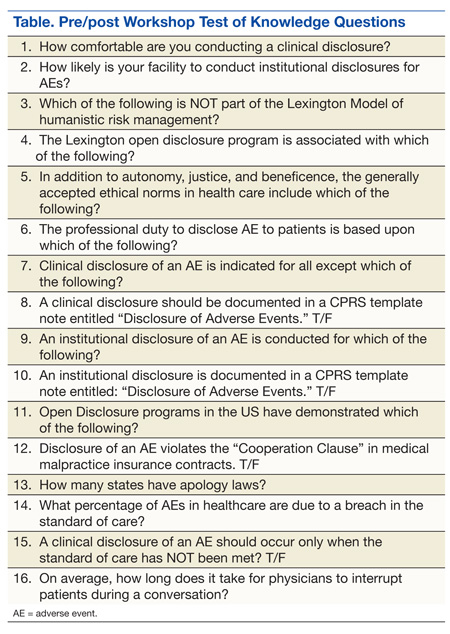
Fourteen workshops were conducted for 346 employees from 26 VAMCs in 2012. Audience response technology was used to elicit participant feedback regarding workshop quality and effectiveness. Additional questions were asked as a pre/post-test of subject matter knowledge. Following the workshop, the participants showed a 30% overall improvement over preworkshop tests (Table), and 95% of participants favorably rated the workshop for quality and effectiveness.
There was a positive association between workshops with facility directors and actively engaged chiefs of staff in attendance and higher improvement scores in the test of knowledge. Among the top 7 performers on this test, 6 were individual facilities hosting the workshops and 1 VISN hosting for several facility representatives. Eleven of the 14 workshops with these characteristics (3 of which included VISN directors) evidenced more than 20% improvement on the test knowledge. These findings confirmed the original program design intended for individual facilities with leadership in attendance.
Iterative improvements were made to the program throughout 2012 based on feedback from workshop attendees, the National Office of Risk Management, the National Center for Ethics in Health Care and participating VA facilities and VISNs.
Despite these encouraging results, the DTP has some significant limitations: It is expensive, labor intensive, and dependent on faculty with expertise in clinical medicine, bioethics, and the law. Considering tight federal budgets, justifying the expenses to host a training program is difficult for a VAMC compared with that of other spending priorities. The actual and opportunity costs of travel to host sites for several facilitators and a group of professional actors to conduct a 2-day workshop for busy HCPs is not trivial.
Another limitation is the use of immediate response technology for data collection. Although this method maximizes response rates and seems to keep attendees engaged in presentations and discussions, technical failures could result in dropped responses, and ultimately the choice to respond is dependent on participant willingness to use the device.
Encouraging results suggest a bright future for the DTP, which has relevance for any health care organization, including the VA, academic affiliates, or those in the private sector. Wherever health care is delivered, providers will have the difficult task of disclosing AEs to meet their duty of care when patients experience harm. Learning empathic communication skills and successful strategies for disclosure will enhance this interaction and contribute to the maintenance of trust that is critical to the provider–patient relationship.
The DTP workshop has a flexible design and can be packaged to accommodate host medical centers for workshops of 1 to 2 days’ duration. The didactic presentations are constant, whereas the number of simulations will vary, depending on the length of the workshop (2-3 simulations for 1 day and 5-7 for two days). Participants from every workshop consistently cite that the simulations with professional actors are a powerful learning experience of significant personal value.
The DTP was developed as a unique, simulation-based program for clinicians, administrators, and allied health care personnel to enhance the effective disclosure of AEs to patients. Feedback from participants in 14 workshops in 2012 cited the value of the program with a high favorability rating. In a test of knowledge, participants also demonstrated an increase in learning. This feedback from the health care professionals who have attended the workshops has validated the pedagogic design of the program, which leverages adult learning principles of learning through experience. This approach was described by Aristotle in his best-known work on ethics, Nicomachean Ethics, “For the things we have to learn before we can do them, we learn by doing them.”15