Dr. Kosasih is a board-certified physiatrist and section chief of the Department of Physical Medicine and Rehabilitation, medical director of the Comprehensive Integrated Inpatient Rehabilitation Program, and medical director of the Polytrauma Clinic Support Team and Amputation Clinic Team; Dr. Hammeke is a board-certified neuropsychologist; Dr. Graskamp is a staff psychologist; and Ms. Owsiany was a psychology technician for the Polytrauma Clinic Support Team at the time of the study; all at the Clement J. Zablocki VAMC in Milwaukee, Wisconsin. Dr. Kosasih also is a professor in the Department of Physical Medicine and Rehabilitation and Dr. Hammeke also is a professor in the Department of Psychiatry and Behavioral Medicine, both at the Medical College of Wisconsin in Milwaukee.
The diagnosis of ADHD in a veteran was established through 1 of 2 methods: (1) report of a developmental history of behavioral adjustment difficulties consistent with ADHD that was coupled with formal psychiatric diagnosis and recommended treatment of ADHD in childhood; or (2) current diagnosis of ADHD as identified in the veteran’s active problem list. In most cases of report of developmental diagnosis, the veteran reported having been diagnosed and having received treatment with a stimulant medication for a period of time. In a few cases, the veteran reported having been diagnosed and stimulant medication was recommended, but the veteran’s parents declined the pharmacologic treatment in favor of behavioral treatment strategies.
In cases of current diagnosis, Diagnostic and Statistical Manual of Mental Disorders, Text Revision, 4th Edition (DSM-IV-TR), criteria were applied and supported by formal clinical examinations for ADHD conducted by psychologists, psychiatrists or neuropsychologists, or through VA disability (Compensation and Pension) evaluations where an issue related to ADHD diagnosis was raised.17 There was considerable overlap between these 2 diagnostic criteria (ie, through report of developmental history of diagnosis or formal adult evaluation) with 93% of cases being positive on both diagnostic methods.
Other comorbid psychiatric (eg, depression, anxiety, PTSD, substance abuse) and medical (eg, headache, pain) conditions also were abstracted from the veteran’s medical records at the time of the intake evaluation. Documentation of these conditions was derived from the veteran’s problem list and clinical notes that identified the condition as a diagnostic conclusion or focus of treatment. The comorbid conditions were not otherwise independently documented. Many veterans were taking psychotropic medications for mood, sleep, or chronic pain problems at the time of evaluation in the PC; however, use of medication and their effects were not systematically evaluated.
Statistical Analysis
In addition to documentation of the population prevalence for ADHD, analysis for disproportionate prevalence of comorbid conditions in individuals with ADHD compared with those without ADHD was done through the use of the chi-square test and/or Fisher exact test. For continuous variables, t tests were used to compare individuals with ADHD with individuals without ADHD. To control family-wise type I error to a P value of .05, a false discovery rate (FDR) was applied to studies of demographics, comorbidities, and ratings of symptomatic distress.
Results
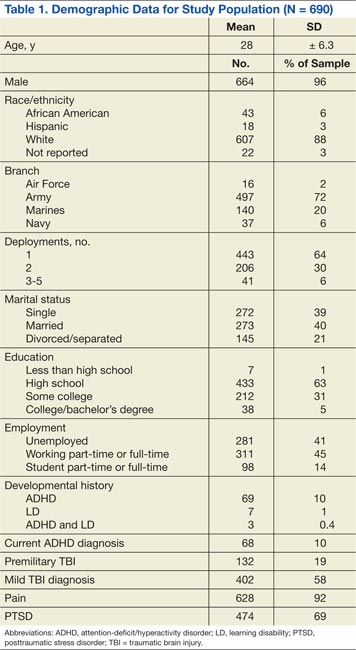
The general population characteristics of the 690 veterans and soldiers are summarized in Table 1. The sample was predominantly male (96%), white (88%), and ranged in age from 22 to 55 years with a mean of 28 years. Active-duty service members and reservists from the U.S. Army, Marines, Navy, and Air Force were represented, but most were Army veterans (72%). Most (63%) had a high school education. About two-thirds of the veterans had a single deployment, and the remaining had multiple deployments.
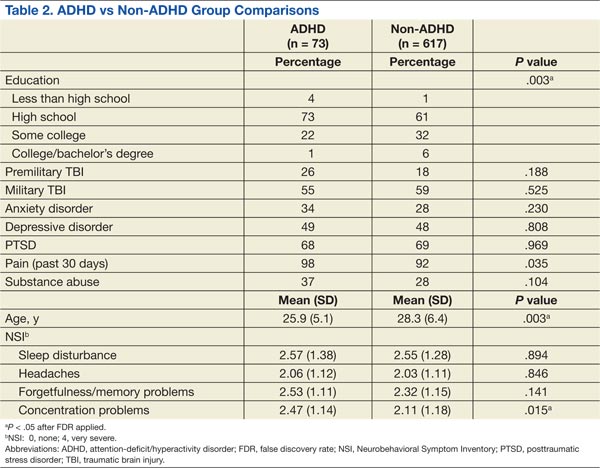
The TBI clinic evaluations found that 58% of the patients had ≥ 1 TBI during their deployments, almost exclusively mild in severity. Seventy-three patients met study criteria for ADHD: 69 with an identified history of diagnosis in childhood and 68 with a current diagnosis, with 93% overlap of these groups. Table 2 provides a breakdown of demographic characteristics, comorbidities, and symptomatic distress in veterans with ADHD compared with those without the diagnosis.
Demographic Characteristics
Veterans with ADHD were found to be slightly younger (2.3 years younger, P = .003) and to have less education (greater frequency of less than high school and high school only, P = .003) compared with those who did not have the diagnosis. No significant group differences in sex, employment/school status, marital status, or number of deployments were identified in veterans with ADHD compared with non-ADHD veterans. Individuals with ADHD did not experience more physical, emotional, or sexual abuse as children than did their non-ADHD counterparts. The prevalence of TBI during deployment was similar in veterans with ADHD compared with that of non-ADHD veterans. There was a trend for veterans with ADHD to have more TBIs prior to military service than in non-ADHD veterans; however, this trend did not reach statistical significance (P = .188).
Comorbidities
After application of the FDR threshold, veterans with ADHD did not show a disproportionate prevalence of mental health diagnoses (eg, PTSD, depression and anxiety disorders, or substance abuse). There was a nonsignificant trend for more veterans with ADHD to report pain during the previous 30 days (P = .035) and more issues with substance abuse (P = .10) than for non-ADHD veterans, but these trends did not meet the FDR threshold of < .05.
Symptomatic Distress
Veterans with ADHD did not report significantly greater levels of distress on either the NSI or the PCLC survey compared with non-ADHD veterans.Not surprisingly, when select symptoms were investigated, veterans with ADHD reported more problems with attention and concentration than for non-ADHD veterans (P = .015). No group differences were identified for sleep issues, headaches, or memory, although there was a trend for the latter (P = .14).