Dr. Khanal and Dr. Upadhyay are third year internal medicine residents, both in the Department of Internal Medicine, and Dr. Silberstein is the division chief of hematology/oncology and professor of internal medicine, all at Creighton University in Omaha, Nebraska. Dr. Silberstein is also the chief of oncology at the VA Nebraska-Western Iowa Health Care System in Omaha, Nebraska.
References
the bottom of the crypt, which migrate upward after division and are eventually shed into the lumen. 16 Each crypt is renewed in 2 to 8 days, which makes colonic mucosa one of the organs with the most cell proliferation in the human body and, hence, a target for various genetic and epigenetic alterations as well as environmental mutagenesis. 7
Traditionally, the majority of colorectal carcinomas were believed to evolve from adenomatous polyps, which transform into an advanced adenoma with high-grade dysplasia and then progress to an invasive cancer often referred to as the adenoma-to-carcinoma sequence. 15 However, 2 other pathways, alternative and serrated, have been described, and CRCs are now regarded as complex malignancies with a wide array of genetic and epigenetic mutations. 17
About 70% to 85% of CRCs generally develop from chromosomal instability resulting from inactivation of tumor suppressor genes (APC gene, p53, etc). About 15% of cases are attributed to the failure of the DNA mismatch repair system either by germline/somatic mutations or by epigenetic silencing of gene transcription by CpG island methylation. 18 Mutation in the BRAF or K-ras oncogenes are also believed to promote carcinogenesis. 15 All these changes are believed to give rise to a precursor microscopic mucosal lesion that precedes the development of macroscopic adenomas. 17
Clinical Features
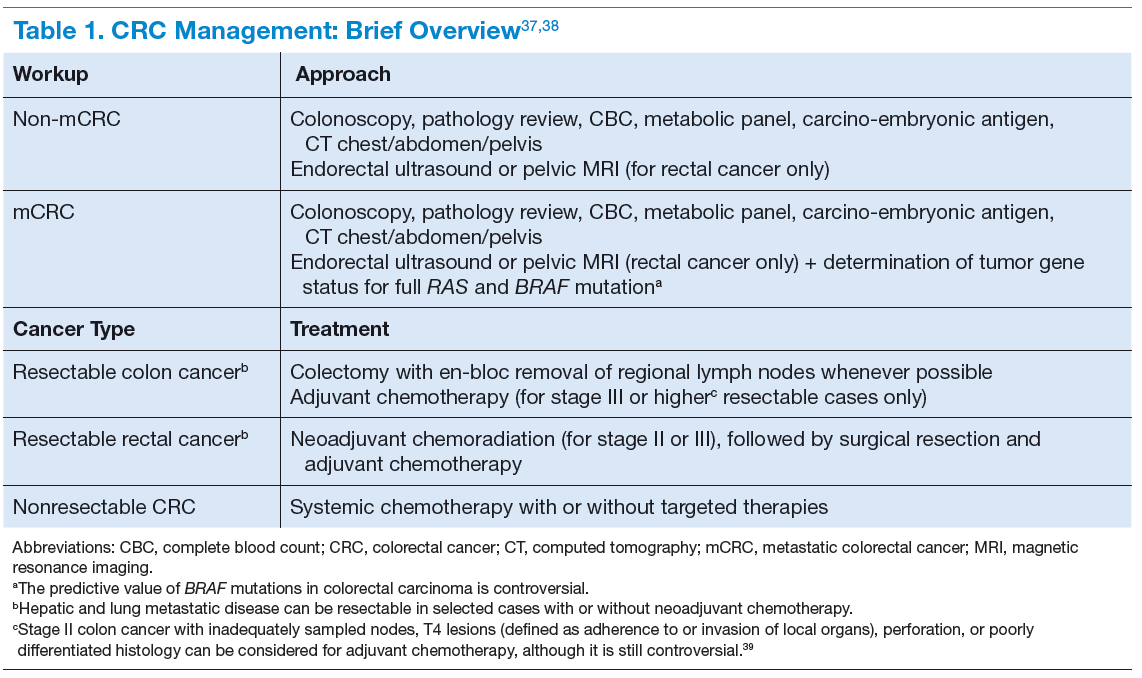
The clinical features of CRCs can be widely variable, from incidental findings during screening colonoscopy to intestinal obstruction. The most common clinical presentation is rectal bleeding, followed by weight loss, abdominal pain, constipation, or diarrhea. 19 The likelihood of CRC is higher with the combination of rectal bleeding and weight loss as well as rectal bleeding and change in bowel habits. Other clinical features may include bloating, abdominal pain, or anemia. 20 (See Table 1.)
Targeted Therapy in CRC
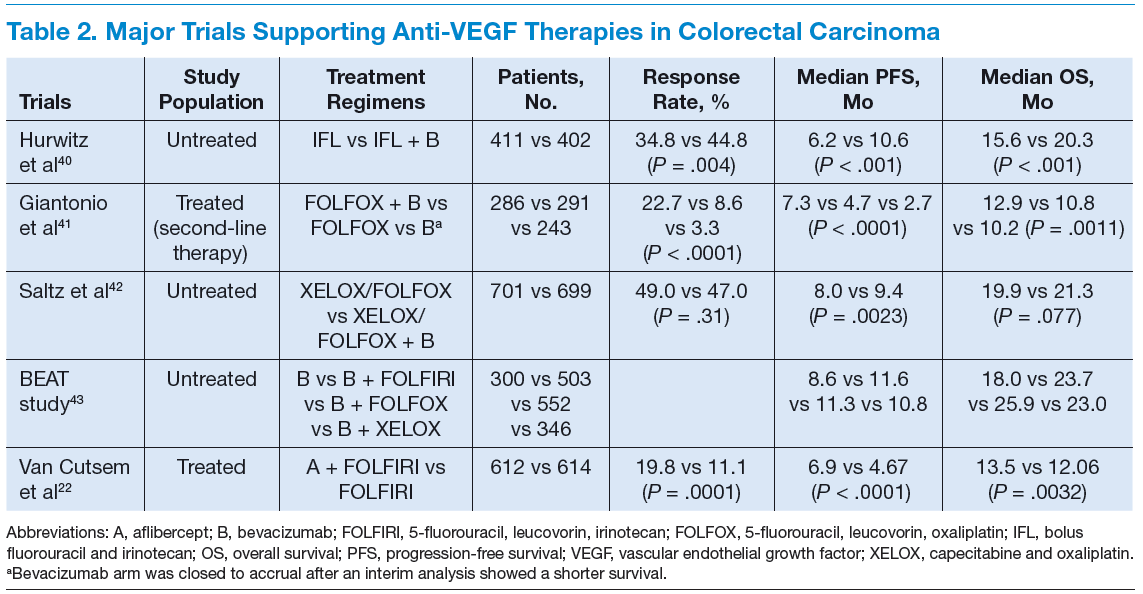
The targeted therapies in CRC include (1) the antivascular endothelial growth factor-A (anti–VEGF-A) antibody bevacizumab; (2) the VEGF-A, VEGF-B, and placental growth factor inhibitor aflibercept; (3) the multikinase inhibitor regorafenib; and (4) the anti-epidermal growth factor receptor (anti-EGFR) antibodies cetuximab and panitumumab.
Bevacizumab is an anti-VEGF monoclonal antibody. Vascular endothelial growth factor promotes angiogenesisnecessary for tumor growth. Bevacizumab was approved by the FDA in February 2004 as a first-line treatment in combination with IFL (irinotecan plus 5-fluorouracil [5-FU]/leucovorin) regimen and in June 2006 as a second-line treatment in combination with 5-FU–based chemotherapy for patients with mCRC. In January 2013, bevacizumab was approved for use in combination with fluoropyrimidine–irinotecan- or fluoropyrimidine–oxaliplatin-based chemotherapy for the treatment of patients with mCRC whose disease has progressed while on first-line treatment with a bevacizumab-containing regimen. 21 (See Table 2.)
Aflibercept is a recombinant fusion protein, containing VEGF-binding