Dr. Gutt is a radiation oncologist at the Washington DC VAMC. Dr. Dawson and Dr. Cheuk are radiation oncologists at the James J. Peters VAMC in the Bronx, New York, and assistant professors at Mount Sinai School of Medicine in New York. Dr. Kelly and Dr. Dawson are radiation oncologists at the New Jersey VAHCS in East Orange, New Jersey. Dr. Fosmire is a radiation oncologist at the Richard L. Roudebush VAMC in Indianapolis, Indiana. Dr. Moghanaki is a radiation oncologist at the Hunter Holmes McGuire VAMC and an assistant professor at Virginia Commonwealth University Massey Cancer Center, both in Richmond, Virginia. Dr. Jolly is a radiation oncologist at the VA Ann Arbor HCS in and an associate professor at the University of Michigan, Ann Arbor.
References
In patients who are not operative candidates, radiation alone is an appropriate alternative. However, several factors need consideration in deciding whether to manage cord compression with surgery followed by RT vs RT alone. These factors include life expectancy, tumor type (myeloma and lymphoma are more radiosensitive), interval since tumor diagnosis, and the presence of visceral metastases. 31 Factors favoring surgical decompression plus postoperative RT over RT alone include spinal instability, KPS (Karnofsky Performance Status) > 70, radio-resistant tumor histology, minimal metastatic disease, and projected survival > 3 months. 10
For patients managed with RT alone, early diagnosis and treatment is associated with improved outcomes. A prospective study of patients treated with RT without surgery for spinal cord compression demonstrated that 82% of patients experienced back pain relief, 76% achieved improvement in or preservation of ambulation, and 44% of patients with sphincter dysfunction experienced improvement with treatment. 32 Patients with certain tumor histologies, such as myeloma, breast cancer, and prostate cancer, had better responses to RT. 32
In the setting of spinal cord compression, longer courses of RT may provide better local control than do shorter courses. 33 Therefore, longer courses of RT, such as 30 Gy in 10 fractions delivered over 2 weeks, are often preferred in cases of spinal cord compression treated with definitive RT as well as after surgical decompression. However, overall life expectancy is an important factor considered by the treating radiation oncologist when selecting a short course vs a longer course of RT.
In the instance of painful vertebral body metastases without spinal cord compression, a new subset analysis of the Radiation Therapy Oncology Group (RTOG) 9714 randomized trial indicated that single fraction RT (8 Gy) is just as effective as multiple fractions (30 Gy in 10 fractions), with this study demonstrating comparable rates of pain relief and narcotic use in both groups 3 months after RT. 34 Advantages to the single-fraction plan compared with those of multiple fractions include mitigation of logistic concerns for patients and family at the end of life and less acute adverse effects.
Brain Metastases
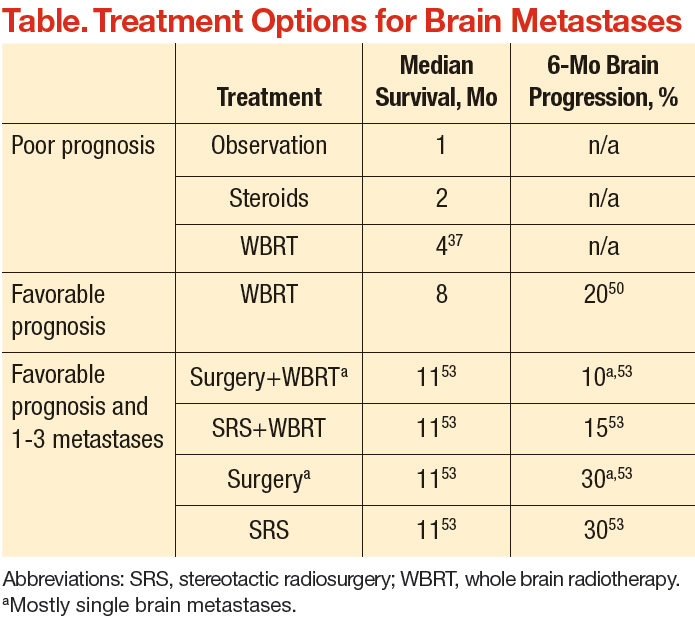
An estimated 20% to 40% of patients with cancer develop brain metastases. 35 The incidence of brain metastases has been rising most likely due to improved detection rates with magnetic resonance imaging (MRI) and improved cancer survival, because treatment regimens have improved with targeted chemotherapy and radiation techniques. Currently, the annual incidence of brain metastases is 170,000 to 200,000 in the U.S. 36 Prognosis for these patients is poor, with median survival of 1 month without treatment and about 4 months with whole brain RT (WBRT) (Table). 25,37-39
The goal of management for patients with brain metastases is to prevent or treat neurologic symptoms and to prolong survival. Treatment options include corticosteroids, WBRT, surgery, and stereotactic radiosurgery (SRS). Recommendations for treatment should involve both a radiation oncologist and neurosurgeon to determine the best treatment for an individual based on patient age, performance status, extent of systemic disease, and number of brain metastases. These prognostic factors that may predict life expectancy and impact treatment recommendations. 40