Just a few years ago, tobacco and alcohol use were presumed to be the main causes of head and neck cancers. Evidence of oropharyngeal cancer associated with human papillomavirus (HPV) first appeared about 10 years ago, but it wasn’t until 2010, with the publication of 2 papers showing far greater survival among HPV-positive patients with head and neck cancer, that oncologists suddenly realized that they were likely dealing with two distinct diseases.
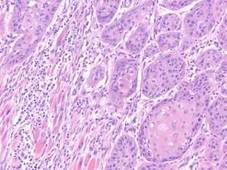 Photo courtesy Tom Carey, Ph.D.
Photo courtesy Tom Carey, Ph.D.
Tissue section from a head and neck cancer patient
“It’s become clear that the disease we thought was one disease related to tobacco and alcohol is now being parsed into two major categories,” Dr. Maura L. Gillison said last week in Phoenix at the 2012 Multidisciplinary Head and Neck Cancer Symposium. At the meeting, she presented her group’s data showing that the overall prevalence of oral HPV infection in people aged 14-69 years is 6.9%, and that the prevalence is much higher among men than women. The Merck-supported trial paper was published online in JAMA on January 26, coinciding with her presentation.
In a separate talk, Dr. Gillison summarized previous work from her group showing that the incidence of HPV-related cancer is rising while HPV-negative cancer is declining, consistent with the decline in tobacco use and changes in sexual behavior that increase HPV transmission. Overall survival of head and neck cancer has improved over the last decade, a trend that is likely due both to the improved prognosis among HPV-positive patients and to the decline in tobacco use rather than to advances in treatment, she said.
This recently heightened role of HPV in head and neck cancer – and the awareness of it - has impacted the field of oncology in several ways. For one, it has dramatically changed the way research is done, conference chair Dr. Ezra Cohen told me. “It has made a tremendous difference in the way clinical trials are conducted, because it makes absolutely no sense to lump these patients together. Now all clinical trials will either stratify for HPV status or design completely separate studies, because they truly are two biologically different diseases.”
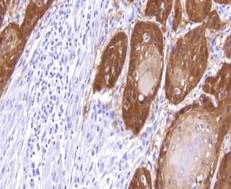 Photo courtesy Tom Carey Ph.D.
Photo courtesy Tom Carey Ph.D.
Tissue section from the same head/neck cancer, with brown stain of an HPV marker protein called p16.
Clinically, patients with head and neck cancers are now routinely tested for HPV. This wasn’t the case prior to 2010. And those who test positive are counseled differently, since their prognosis is better. Indeed, Dr. Cohen said, HPV-positive head/neck cancer patients appear to respond better to just about every type of treatment, including surgery.
What’s more, Dr. Gillison told me, HPV has essentially upended some of the tools oncologists use to predict outcomes in head and neck cancer patients. One example is the current tumor staging system, which doesn’t take into account HPV status. A Stage 3 or 4 cancer which carries a poor prognosis among HPV-negative patients might carry the prognosis now associated with Stage 1 cancer among those who are HPV-positive. And another factor that has been shown to predict poor outcome in HPV-negative patients, the presence of extracapsular extension, appears to have little impact in those who are HPV-positive.
“So all these things that we take as firmly established and drivers of treatment decisions in this new setting are all in question,” she said.
Thus far there have been no major changes in treatment, but Dr. Cohen believes that is likely to change as more data become available. He is currently leading a clinical trial in collaboration with Novartis Pharmaceuticals looking at treatment with reduced radiation doses – and thereby reduced toxicity - for patients who have a good response to induction chemotherapy. Such patients are usually HPV positive.
Another study, funded by the National Cancer Institute, randomizes HPV positive patients to radiation combined with either chemotherapy or a monoclonal antibody, with the hypothesis that the latter will be better tolerated.
Dr. Cohen cautioned that treatment changes won’t come immediately. “Many of us in the field believe that there will be different therapies developed for [HPV-positive] patients, but it takes time to do that. It’s hard to make those changes, especially when we are curing the majority of these patients.”
-Miriam E. Tucker (@MiriamETucker on Twitter)