An oral inhibitor of respiratory syncytial virus replication, currently called ALS-008176, significantly reduced total viral load, peak viral load, duration of viral shedding, and clinical symptoms in a small proof-of-concept study funded by the drug’s manufacturer and published online Nov. 18 in the New England Journal of Medicine.
These findings are particularly encouraging because at present, the standard of care for RSV infection is limited to supportive care only, said Dr. John P. DeVincenzo of the departments of pediatrics, microbiology, immunology, and biochemistry, University of Tennessee, and the Children’s Foundation Research Institute at Le Bonheur Children’s Hospital, both in Memphis.
 ©Dr. Craig Lyerla/CDC
©Dr. Craig Lyerla/CDC
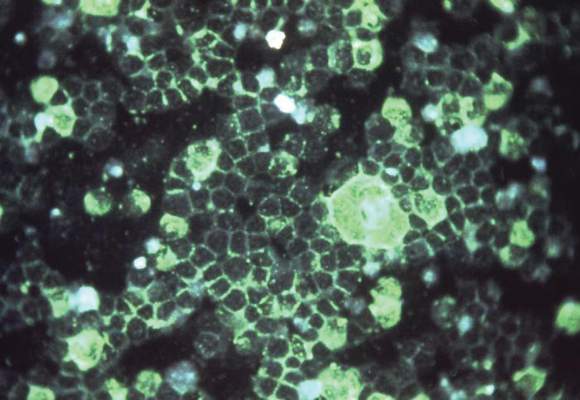
This is the photomicrographic detection of respiratory syncytial virus (RSV) using indirect immunofluorescence technique. RSV is the most common cause of bronchiolitis and pneumonia among infants and children under 1 year of age. The majority of childre
Dr. DeVincenzo and his colleagues performed this randomized, double-blind trial during three separate study periods in which up to 22 healthy adults were confined to a special quarantine unit for 2 weeks at a time. All 62 participants were inoculated intranasally with a clinical strain of RSV and monitored twice daily for the development of RSV infection via assays of fresh nasal washings. The participants were randomly assigned to receive the first dose of ALS-008176 or a matching placebo about 12 hours after the detection of RSV, or on the morning of day 6, whichever came first.
The active drug or the placebo were administered orally every 12 hours for 5 days, for a total of 10 doses. Three dosing regimens were assessed: In the first study period, participants were given a single loading dose of 750 mg followed by nine maintenance doses of 500 mg; in the second period, participants were given a single loading dose of 750 mg followed by nine maintenance doses of 150 mg; and in the third period, participants were given 10 doses of 375 mg each. A total of 35 study participants developed RSV infection.
Compared with placebo, all three dosing regimens significantly reduced viral load within 12 hours of starting treatment: by 88.0% in the first study period, by 85.3% in the second, and by 73.4% in the third. The mean interval until RSV RNA became undetectable ranged from 1.3 to 2.3 days for the three active-treatment groups, compared with 7.2 days for placebo. RSV RNA became undetectable within 4.5 days for all participants who received ALS-0081, compared with 11 days for those who received placebo.
In addition, mean peak viral loads were lower for all three dosing regimens than for placebo. “At the time that the peak viral load occurred in the placebo group, the mean viral load in each of the 3 ALS-008176 treatment groups was more than 1,000 times as low,” wrote Dr. DeVincenzo and his associates (N Engl J Med. 2015 Nov 19;373:2048-58. doi:10.1056/NEJMoa1413275).
As important, RSV symptoms were much less severe in all three active-treatment groups than in the placebo group, as assessed subjectively via symptom scores and objectively via the quantity of nasal mucus produced.
The small study population limited the ability to detect potential safety concerns. Nevertheless, “no serious adverse events, premature discontinuation of the study drug, or clinically significant, treatment-related adverse events were observed in any participants in the intention-to-treat population,” the investigators added.
They noted that people who are infected with RSV under natural circumstances, particularly infants, typically present later in the course of the disease, only after patients or caregivers realize that the illness is not due to a simple cold. Thus, their disease severity would be worse than that of these study participants by the time ALS-008176 could be administered. “Therefore, it may be inappropriate to directly extrapolate the results of this study to a clinical setting,” Dr. DeVincenzo and his associates said.
Alios BioPharma, maker of ALS-008176, funded the study. Dr. DeVincenzo disclosed ties with Alios BioPharma, Gilead Sciences, Alnylam Pharmaceuticals, Microdose Therapeutx–Teva, Janssen, ADMA Biologics, and MedImmune/AstraZeneca. His associates reported ties to Alios and Retroscreen Virology.