PASADENA, Calif. – Dermatologists tend to use too many different names for a single entity with a defined clinical spectrum—toxic erythema of chemotherapy.
 Courtesy of Dr. Jean Bolognia
Courtesy of Dr. Jean Bolognia
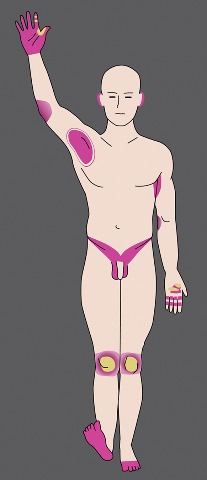
Toxic erythema of chemotherapy appears in a several sites on the body.
“We have too many names for one disease,” and this complicates clinical communication and decisions about management, Dr. Jean Bolognia said at the annual meeting of the Pacific Dermatologic Association.
If dermatologists used the term “toxic erythema of chemotherapy” (TEC), they would improve discussions with hematologists, oncologists, and internists, said Dr. Bolognia, professor of dermatology at Yale University, New Haven, Conn. Other terms sometimes used in place of TEC (see list below) include eccrine squamous syringometaplasia and epidermal dysmaturation. While some alternative terms may be histologically accurate, they can be confusing to nondermatologists as diagnoses.
The term TEC indicates that the patient is not having an allergic reaction or an infectious process. It tells clinicians that the dermatologic problem will resolve spontaneously but can recur if the patient again uses a similar or higher dosage of the drug that caused it, noted Dr. Bolognia.
Cytarabine (Ara C) and anthracyclines are “at the top of the list” of drugs associated with TEC, so patients with acute myelogenous leukemia commonly develop TEC. The liposomal form of doxorubicin is “kinder and gentler when it comes to your bone marrow and your hair, but is worse when it comes to producing TEC,” she said.
Other drugs most commonly associated with TEC include taxanes (often used to treat breast cancer), methotrexate, multikinase inhibitors, gemcitabine, clofarabine, pralatrexate, 5-fluorouracil (5-FU), and prodrugs that turn into 5-FU in the body (like capecitabine).
Busulfan, until recently, was an oral chemotherapeutic drug that caused nausea and vomiting, which lead to underdosing. Now that it is administered intravenously, it is more likely to give rise to TEC, she said. If called upon to evaluate a possible case of erythema multiforme, Stevens-Johnson syndrome, or toxic epidermal necrolysis in a patient who has received IV busulfan in the past several weeks, consider TEC.
Clinically, signs and symptoms of TEC can occur a month or so after the drug is given. TEC appears as erythematous or violaceous patches or edematous plaques. “They’re going to appear on hands and feet, elbows and knees, axillae and groin, including the scrotum, and occasionally on the ears,” she said. When it’s severe, a good portion of the skin surface can have the appearance of a sunburn.
Once you know the distribution pattern for TEC bullae “you can make the diagnosis at the bedside,” she added.
The lesions are associated with pain and burning more than with pruritus, suggesting a toxic reaction. Their dusky hue can contribute to misdiagnoses, such as toxic erythema multiforme, Stevens-Johnson syndrome, or toxic epidermal necrolysis.
The lesions may become purpuric, especially in the setting of thrombocytopenia, leading to the misdiagnosis of vasculitis. Sterile bullae followed by erosions also develop within the plaques, followed by desquamation and spontaneous resolution regardless of the therapy chosen. Of note, the desquamation is dry on the palms and soles or elbows and knees, but is moist in the major body folds.
 Courtesy of Dr. Jean Bolognia
Courtesy of Dr. Jean Bolognia
Toxic erythema can appear as violaceous patches or edematous plaques on the knees.
Dr. Bolognia said she would especially like to see dermatologists stop using the term “acral erythrodysesthesia,” or “hand-foot syndrome,” because patients often have additional sites of involvement and trying to explain the cutaneous findings in these areas can lead to erroneous diagnoses. For example, the lesions on the elbows and knees may be misdiagnosed as dermatitis or involvement of the axillae and groin as cutaneous candidiasis, even though the patient is already receiving voriconazole.
“By simply saying you have TEC, you have a unifying diagnosis,” she said. “Histologic findings include atypia and apoptosis of keratinocytes, as well as some loss of polarity of epidermal cells and crowding of keratinocytes. There is vacuolar degeneration of the basal layer, which may lead the dermatopathologist to raise the possibility of erythema multiforme, Stevens-Johnson syndrome, or graft-versus-host disease.”
Additional findings include eccrine squamous syringometaplasia and eccrine hidradenitis. Distinguishing TEC from graft-versus-host disease or erythema multiforme/Stevens-Johnson syndrome superimposed upon chemotherapy-induced changes may be difficult histologically, but the dermatologist can do the clinicopathologic correlation and arrive at the diagnosis, she said. For example, on the palmar surface of the hands, a clinical clue to the diagnosis of TEC is accentuation of erythema and bullae within the creases of the digits, a finding not seen in the differential diagnoses.