Strict heart rate control has no benefit over more lenient control in patients with atrial fibrillation, experts stated in an update of treatment guidelines. The update, which contained several new recommendations for the management of atrial fibrillation, was published online Dec. 20 in Circulation.
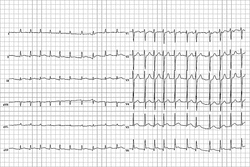 Photo credit: Steven Fruitsmaak via Wikimedia Commons
Photo credit: Steven Fruitsmaak via Wikimedia Commons
ECG from a man with bradycardia-tachycardia syndrome shows atrial fibrillation at 126 beats per minute. New guidelines update the management of atrial fibrillation.
The previous guidelines advised keeping the heart rate of an atrial fibrillation patient at less than 80 beats/min at rest and less than 110 beats/min during a 6-minute walk. The updated guidelines advise keeping a resting heart rate of less than 110 beats/min in patients with persistent atrial fibrillation who also have stable ventricular function and have no symptoms, or symptoms deemed acceptable, related to their arrhythmia.
The 2011 Focused Update on the Management of Patients With Atrial Fibrillation (Updating the 2006 Guideline) is a joint effort of the American College of Cardiology Foundation, the American Heart Association, and the Heart Rhythm Society. The guideline writing committee reviewed data from late-breaking clinical trials presented at scientific sessions of the AHA, ACC, and European Society of Cardiology in 2009, and other data published through April 2010 (Circulation 2010 [doi:10.1161/CIR.0b013e3181fa3cf4]).
Another key update is the recommendation that a combination of clopidogrel and aspirin might be an option for atrial fibrillation patients who are poor candidates for warfarin. The recommendation is based on recent studies including the ACTIVE-A trial (Effect of Clopidogrel Added to Aspirin in Patients with Atrial Fibrillation). In this study, significantly fewer major vascular events occurred in patients randomized to receive clopidogrel plus aspirin, compared with those who received aspirin plus placebo.
"The clopidogrel/aspirin option is going to be of limited utility in most cases," commented Dr. Anne B. Curtis, who was a member of the writing group, in an interview. The new thrombin inhibitors such as dabigatran will be used instead, she said. Because dabigatran was not approved by the Food and Drug Administration when the committee was making its decisions, it was not included in the guidelines, according to the report.
The updated guidelines also suggest the use of dronedarone for some atrial fibrillation patients to reduce hospitalizations for cardiovascular events. Recent studies such as the DIONYSOS study (Efficacy and Safety of Dronedarone Versus Amiodarone for the Maintenance of Sinus Rhythm in Patients With Persistent Atrial Fibrillation) showed that dronedarone was less effective than amiodarone for reducing the recurrence of atrial fibrillation. However, in a placebo-controlled, double-blind, parallel-arm trial to assess the efficacy of dronedarone 400 mg b.i.d. for the prevention of cardiovascular hospitalization or death from any cause in patients with atrial fibrillation/atrial flutter (the ATHENA trial), dronedarone reduced the "the combined end point of death and cardiovascular hospitalizations, largely by reducing hospitalizations related to atrial fibrillation," the reviewers wrote. However, dronedarone should not be given to patients with NYHA class IV heart failure or patients with decompensated heart failure within the past 4 weeks, they noted.
To maintain normal sinus rhythm, the updated guidelines support the use of catheter ablation based on data from more than 6,900 patients. In one multicenter study (the ThermoCool trial), symptomatic patients with paroxysmal atrial fibrillation who were treated with catheter ablation showed significant improvement after 3 months, compared with control patients. Currently, catheter ablation treatment is recommended for atrial fibrillation patients without severe lung disease who have not had success with drug therapy.
Dr. L. Samuel Wann, a cardiologist at Wheaton Franciscan Healthcare in Wauwatosa, Wis., served as chair of the 2011 Writing Group Committee. Dr. Wann and his colleagues wrote that the 2006 full-text guidelines for the management of atrial fibrillation that are not mentioned in the 2011 update remain unchanged at this time. "The guidelines attempt to define practices that meet the needs of most patients in most circumstances," the reviewers said.
"The last time the guidelines were published was in 2006, and there have been several new drugs and treatments that have been developed since that time. Physicians want to know where they stand in terms of the hierarchy of treatment of patients with atrial fibrillation," explained Dr. Curtis, chair of the department of medicine at the University of Buffalo, N.Y. "In order to be timely, we did a limited, focused update," she said.
The clinical implications of more lenient heart rate control are unclear at this time, Dr. Curtis said. In the Rate Control Efficacy in Permanent Atrial Fibrillation (RACE II) study, on which the recommendations were based, the difference in heart rate control between lenient control and strict control groups was limited, she noted.