The American Heart Association for the first time released guidelines for clinicians to help detect and treat cerebral venous thrombosis, a rare stroke that disproportionately affects young people, especially women who are pregnant or on oral contraceptives, or who just gave birth.
 Courtesy of Dr. Gustavo Saposnik
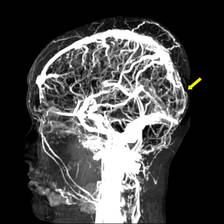
Courtesy of Dr. Gustavo Saposnik
Magnetic resonance venography shows thrombosis of the superior sagittal sinus.
The guidelines include an algorithm for diagnosing and managing cerebral venous thromboembolism (CVT), which is caused by a clot in the dural venous sinuses, veins that drain blood from the brain toward the heart. The guidelines were released Feb. 3 online in advance of publication in Stroke.
CVT is difficult to recognize because of its diverse risk factors and presentations. "The diagnosis and management of CVT requires a high level of suspicion," Dr. Gustavo Saposnik said in an e-mail interview. Dr. Saposnik, codirector of the stroke program at the University of Toronto, chaired the guidelines writing committee of nine experts from five countries, which reviewed the literature on CVT and rated the evidence behind their recommendations (Stroke 2011 Feb. 3 [doi:10.1161/STR.0b013e31820a8364]).
The guidelines have been endorsed by the American Academy of Neurology, the American Association of Neurological Surgeons, the Congress of Neurological Surgeons, the Society of NeuroInterventional Surgery, and the Ibero-American Stroke Society.
Many kinds of physicians may be the first to encounter a patient with CVT because of its many causes and symptoms. The guidelines should be helpful not only to neurologists but also to emergency physicians, internists, family physicians, obstetricians, oncologists, pediatricians, hematologists, and more, he said.
Approximately five people per million develop CVT each year, accounting for 0.5%-1% of all strokes. In the largest cohort study of patients diagnosed with CVT, 54% were on oral contraceptives, 34% had an inherited or acquired prothrombotic condition, and 21% were pregnant or in the immediate postpartum period. Other predisposing conditions included infection in 12%, the presence of certain drugs in 8%, cancer in 7%, and other hematologic disorders in 12%. (Some patients had more than one predisposing condition.)
Patients may present with slowly progressive symptoms, and delays in diagnosis are common. Studies have reported a mean lapse of 4 days from onset of symptoms to hospital admission, and 7 days from onset of symptoms to diagnosis. Headache, the most common symptom, occurs in about 90% of cases. Seizures also are common.
Approximately 30%-40% of patients with CVT present with intracranial hemorrhage. To select the appropriate treatment, it is important to identify CVT as the cause of the hemorrhage, instead of a ruptured brain artery or other causes.
Women outnumber men with CVT at ages younger than 61 years. The largest cohort study of CVT reported that patients younger than 50 years accounted for 78% of cases. The incidence of CVT during pregnancy and post partum in Western countries ranges from one to four cases per 10,000 deliveries, with the greatest risk during the third trimester and in the first 4 weeks after delivery.
CVT is not a contraindication for future pregnancy, Dr. Saposnik said.

Dr. Gustavo Saposnik
If a clinician suspects CVT, either MRI or magnetic resonance venography (MRV) is recommended to make the diagnosis by showing a thrombus obstructing the venous sinuses or cerebral veins. In emergency departments, either a CT scan or CT venography can be used if MRI is not available. "This allows different clinicians to initiate the appropriate work-up in the acute setting," Dr. Saposnik said.
Anticoagulation is the usual first-line therapy, with IV heparin or subcutaneous low-molecular-weight heparin in patients without contraindications. "There are several things that we still don’t know. For example, the anticoagulation regimen and duration of IV anticoagulation therapy is not clear," he said.
There is only limited, low-grade evidence for alternative treatments, such as endovascular therapy or decompressive hemicraniectomy. "These should be reserved for patients with progressive neurological deterioration despite anticoagulation therapy and the best medical treatment," Dr. Saposnik said.
A randomized trial is underway comparing anticoagulation therapy with endovascular thrombolysis to treat CVT.
One guidelines coauthor reported a financial relationship with Boehringer Ingelheim, and another reported being an adviser or consultant for Servier and Tecnifar. Another coauthor received less than $10,000 as an expert witness in a legal case concerning CVT. Disclosures of funding for the American Heart Association can be read online.