DETROIT – Chest wall reconstruction that uses nonrigid mesh or autologous tissue without rigid fixation was safe and provided excellent respiratory outcomes in one of the largest series to date.
"Our recommendations are to reconstruct with autologous tissue alone whenever possible," Dr. Waël Hanna said. "If you have to use mesh because you cannot reapproximate the chest wall or there’s not enough muscle to construct a flap, then nonrigid mesh should be favored over rigid fixation."
 Photo courtesy of Dr. DS Mulder
Photo courtesy of Dr. DS Mulder
These images illustrate the steeps of resection and reconstruction of the chest wall. Pictured here is the chest wall defect after resection.
Rigid fixation with methacrylate or metallic plates and screws has conventionally been advocated as the best method to achieve chest wall stability and to maintain respiratory integrity following resection of chest wall tumors. However, these approaches are frequently complicated by motion deformities of the shoulder girdle, long-term cosmetic deformities, pain that limits daily activities, and a high morbidity of infection, Dr. Hanna explained at the annual meeting of the Central Surgical Association.
He reported on 37 patients who underwent major chest wall reconstruction in 2003-2010 with autologous tissue alone or with a soft prosthetic mesh. No patient underwent rigid fixation with methacrylate or plates and screws. The study excluded patients with concomitant lung or pleural resection to avoid confounding the respiratory outcomes.
Nine patients had a small defect (less than 60 cm2) and 28 patients had a large defect (greater than 60 cm2); no defect measured exactly 60 cm2, according to Dr. Hanna. The large-defect group was further divided into a subgroup of 16 patients who were reconstructed with soft mesh alone and a subgroup of 12 patients whose reconstruction was with autologous tissue alone and no mesh. Soft mesh was used in only one small-defect patient.
"We have turned away from using rigid prosthetics or methacrylate at our institution," said Dr. Hanna, a fifth-year resident with McGill University in Montreal.
Sarcoma was the most common indication for resection, followed by metastases to the chest wall, neurofibromas, and desmoid tumors. Reconstruction parameters were similar between the small- and large-defect cohorts, except for the mean size of the defect that was created in the chest wall (51 cm2 vs. 149 cm2), the dissection of three or more ribs (0% vs. 50%), and the use of soft mesh only (11% vs. 61%). A muscle flap to cover the prosthesis was used equally in both cohorts (56% vs. 75%).
The rate of immediate postoperative extubation was similar, at 100% in the small-defect cohort and 89% in the large-defect cohort, Dr. Hanna said. Only one patient was reintubated on postop day 1 and remained intubated for 3 days in the ICU.
None of the small-defect group went to the ICU for ventilation or flap monitoring, whereas 11% and 18% of the large-defect cohort did (P = .006 for both subgroups).
Pneumonia developed in three patients with large defects and in none with small defects (11% vs. 0%). One patient had to be re-extubated postoperatively, he said.
Secondary outcomes were also similar between the small- and large-defect groups, including site infection (0% vs. 7%) and reoperation rates (0% vs. 11%).
A subgroup analysis comparing patients with and without mesh revealed no significant differences in the primary outcomes of immediate extubation (100% vs. 75%), ICU stay for ventilation (6% vs. 25%), ICU stay for flap monitoring (13% vs. 17%), or pneumonia (6% vs. 8%).
The mesh and no-mesh subgroups were also nonsignificantly different with regard to site infection (13% vs. 0%) and reoperation (19% vs. 0%).
After a mean follow-up of 42 months (range, 36-84 months), there were no reports of infections beyond 30 postoperative days, long-term pain, restriction of mobility, or cosmetic disturbances. Patients were seen every 3 months for the first 2 years and every 6 months thereafter.
"For chest wall defects smaller than 60 cm2, reconstruction without a prosthesis has excellent outcomes," Dr. Hanna concluded. "For [defects] larger than 60 cm2, there does not seem to be any major difference between autologous tissue alone vs. nonrigid prosthesis reconstruction.
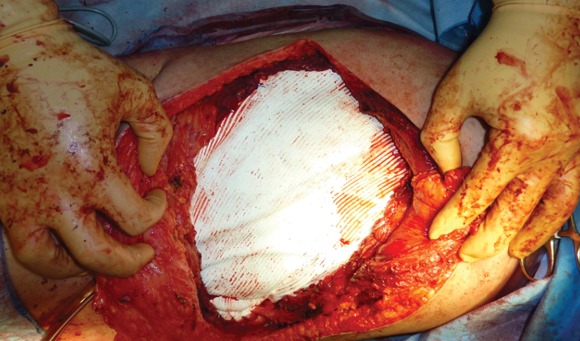 Photo courtesy of Dr. DS Mulder
Photo courtesy of Dr. DS Mulder
This shows the closure with Gore-Tex mesh.
"Finally, nonrigid mesh seems to offer better short-term and long-term outcomes," compared with the historical data on rigid fixation, he said.
Invited discussant Dr. Fred Luchette, professor of surgery at Loyola University Medical Center in Chicago asked how the surgeons manage the often catastrophic event of mesh infection, and whether any long-term pulmonary function data were available, as the defects would likely prompt the development of some degree of paradoxical chest wall motion, even with the soft mesh.