Endometriosis is a prevalent disease that affects 10%-15% of women of reproductive age. In 1990, investigators in Belgium first described deep endometriosis to highlight the diagnostic and therapeutic aspects of the disease (Fertil. Steril. 1990;53:978-83). In contrast to superficial disease, deep endometriosis constitutes the most severe form of endometriosis and includes nodules affecting the pouch of Douglas, retrocervical area, bladder, ureter, or the intestinal wall. Less frequently, the rectovaginal septum is involved (Arq. Gastroenterol. 2003;40:192-7). The treatment of bowel endometriosis is challenging, as it is a benign disease that may infiltrate the bowel, requiring a surgical treatment with increased risks.
Preoperative Diagnosis Using Imaging
The definitive diagnosis of deep endometriosis with bowel involvement is reached principally at the time of surgery. However, some clinical characteristics identified by history and physical examination, laboratory tests, and diagnostic imaging may raise suspicion for this form of endometriosis. A surgical approach is still recommended for confirmation and treatment.
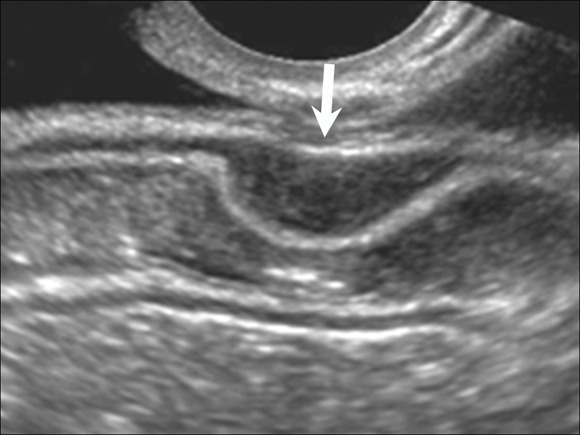 Photo courtesy Dr. Mauricio S. Abrão
Photo courtesy Dr. Mauricio S. Abrão
Figure 1. Transvaginal ultrasound is show with a hypoechoic lesion compromising the inner muscularis of the rectum.
Transvaginal ultrasonography (TVUS) still appears to be the superior imaging technique, providing the best cost-benefit ratio for cases of ovarian or deep endometriosis. The presence of a hypoechoic lesion located in the posterior pelvic compartment is suggestive of endometriosis, with diagnostic sensitivity greater than 95% for retrocervical lesions and greater than 98% for rectal lesions (Hum. Reprod. 2007;22:3092-7).
When performed after complete bowel preparation and during the perimenstrual phase, TVUS carried out by a trained professional provides useful information for therapeutic management.
MRI can be performed to identify deep lesions. It provides a good map of the pelvis, but with lower accuracy than TVUS offers in predicting the depth of involvement of a bowel compromised by endometriosis. Similarly, opaque barium enema does not have a high degree of accuracy; its sensitivity is only 54%. Rectosigmoidoscopy or colonoscopy may be necessary to investigate the involvement of the intestinal lumen and to check other concomitant pathologies; however, this procedure has an estimated sensitivity of 51% and is frequently negative even in the presence of extensive intramuscular deposits of endometriosis.
Excretory urography or uro-MRI also is useful for evaluating whether the ureters are involved. When urinary tract involvement is suspected, one of these types of imaging should be performed to fully document the state of the urinary tract before surgery.
If we have doubts about the bowel involvement even after TVUS with bowel preparation, we recommend rectal echoendoscopy. This was initially used for staging cases of rectal neoplasia prior to surgical treatment. Dr. T. Ohba and his associates in Japan were the first to use this tool to evaluate patients with endometriosis of the rectovaginal septum, using a linear transducer (Hum. Reprod. 1996:11:2014-7). They described how the presence of irregular images, when associated with clinical symptoms, was suggestive of endometriosis.
Rectal echoendoscopy also permits identification of the distance between the lesion and the rectal lumen, as well as identification of extrinsic compression and lesions of the rectal submucosa. This information can be critical in the preoperative planning of the type of surgery required and the need to have the help of a colorectal surgeon.
Treatment: Clinical or Surgical?
Medical treatment of deep endometriosis, as opposed to surgical treatment, remains controversial. Dr. Luigi Fedele and his associates in Italy reported a substantial improvement in pain during 6 months of treatment with GnRH analogs (Am. J. Obstet Gynecol. 2000;183:1462-7). Similar improvements in pain were also observed by our group with both an intrauterine device medicated with levonorgestrel and with a GnRH analog (Hum. Reprod. 2005;20:1993-8). In Dr. Fedele’s study, however, an early relapse occurred following discontinuation of treatment. In addition, the endometriotic lesions underwent a discrete but significant reduction in size as detected by TVUS during treatment, but returned to their original size 6 months after suspension of GnRH treatment.
In cases of intractable pain (measured by scores greater than 7 in the visual analog scale) and/or two previously failed IVF (in vitro fertilization) cycles, surgical treatment is required. Access for surgical treatment may be by laparotomy or laparoscopy, depending on the surgeon’s experience; however, laparoscopy can provide a better visualization of the lesions, allowing a more precise excision.
Surgical Preparation and Technique
Whenever there is clinical suspicion of deep endometriosis, adequate presurgical bowel preparation is indicated. We recommend the use of 3-4 liters of an oral solution of polyethylene glycol (PEG) the day before surgery, followed by one or two Fleet enemas or a mannitol preparation. Administration of antibiotics should be carried out during anesthetic induction, preferably using a second-generation cephalosporin (2 g intravenously).