A pharmacotherapeutic approach that harnesses the amyloid-beta clearing effects of the apolipoprotein E gene while also activating microglia to clear amyloid plaques from the brains of mouse models of Alzheimer’s disease could become a new treatment strategy to test clinically.
The protein product of the APOE gene – the most influential genetic risk factor for late-onset Alzheimer’s disease in humans – normally acts to help build high-density lipoprotein (HDL) particles that promote the degradation of soluble forms of amyloid-beta, which is thought by many researchers to cause the cognitive dysfunction associated with Alzheimer’s. However, efforts that seek to induce the expression of the APOE gene must also ensure that its protein product is lipidated by associated proteins in order for it to clear soluble amyloid-beta.

Gary E. Landreth, PhD.
Paige E. Cramer and Gary E. Landreth, Ph.D., of Case Western Reserve University, Cleveland, and their colleagues took that approach in experiments by inducing the expression of APOE in mouse models of Alzheimer’s disease with the retinoid X receptor agonist bexarotene (Targretin). The drug already is approved by the Food and Drug Administration for the treatment of cutaneous T-cell lymphoma; it is known to cross the blood-brain barrier and has a favorable safety profile.
The investigators used an agonist of the retinoid X receptor (RXR) because the receptor increases the expression of APOE and the lipid transporters ABCA1 and ABCG1 while also stimulating the secretion of highly lipidated HDL particles that are necessary for the clearance of soluble amyloid-beta. RXR agonists such as bexarotene also convert microglia and macrophages into an alternative activation state that helps to clear amyloid-beta plaques.
Unlike interventional approaches to Alzheimer’s therapy that have used vaccines or inhibitors of beta- and gamma-secretase, Dr. Landreth and his colleagues stimulated the normal, physiological clearance mechanisms for soluble amyloid-beta and amyloid-beta plaques.
“There’s no precedent for this,” Dr. Landreth said in an interview.
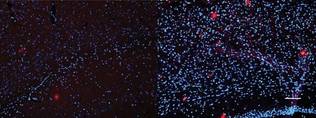 Photo (c)Science/AAAS
Photo (c)Science/AAAS
Significantly fewer amyloid-beta plaques (red) remain in the cortex of a 6-month-old mouse model of Alzheimer's disease after a 14-day period of treatment with bexarotene (left image) than after placebo treatment (right).
Dr. Landreth emphasized that the oncologically effective dose that they used in the experiments is “way too high to treat Alzheimer’s disease or other CNS diseases,” noting that “it may be unsafe to administer this drug to an AD patient at anywhere near the dosages we’ve reported.”
Within 24 hours of giving bexarotene to transgenic mice expressing mutations in several genes known to be associated with early-onset Alzheimer’s in humans, the investigators found that brain interstitial fluid levels of amyloid-beta had dropped by 25%, followed by a return to baseline by 84 hours. However, the drug had no effect on amyloid-beta levels in mice bred without APOE, which indicated that the clearance of amyloid-beta required APOE (Science 2012 Feb. 9 [doi:10.1126/science.1217697]).
During a 14-day treatment period, the investigators observed a sustained 30% reduction in soluble amyloid-beta levels and a 75% reduction in amyloid-beta plaques. They also found abundant microglia laden with amyloid-beta beginning 3 days after treatment with bexarotene, as well as a progressive enhancement of the expression of APOE, ABCA1, ABCG1, and elevated HDL levels in the hippocampus and cortex of the mice.
Treatment of older, 11-month-old mice with greater plaque deposition, compared with 2- and 6-month-old mice, led to significantly reduced levels of both soluble and insoluble amyloid-beta as well as a 50% decline in the number of plaques and a simultaneous increase in the expression of APOE, ABCA1, and ABCG1 and HDL levels.
Although soluble amyloid-beta levels were continuously reduced during a 3-month period of daily treatment with bexarotene, the researchers surprisingly found no change in amyloid plaque burden at the end of treatment. This raises the question, “Do plaques matter?” Dr. Landreth said.
Treatment with bexarotene also restored cognition and memory in both 6- and 11-month-old transgenic mice during treatment periods lasting 7 days and 3 months.
“The ability of bexarotene to rapidly reverse a broad range of deficits suggests that RXR agonists may be of therapeutic utility in the treatment of AD and its antecedent phases,” Dr. Landreth and his associates wrote.
They plan to perform additional preclinical work to determine how small of a dose of bexarotene is necessary to get the same effects observed in the experiments. This will help to determine what dose to give to normal human subjects in a pilot, proof-of-mechanism clinical study that Dr. Landreth said he and his colleagues would like to conduct in the next few months.
Dr. Landreth and Ms. Cramer hold a U.S. provisional patent application for bexarotene as a potential therapy for Alzheimer’s disease and have founded ReXceptor Inc. The researchers received support from the Blanchette Hooker Rockefeller Foundation, the Thome Foundation, the Roby and Taft Funds for Alzheimer’s Research, the National Institutes of Health, the Charles F. and Joanne Knight Alzheimer’s Disease Research Center at Washington University in St. Louis, and the Marian S. Ware Alzheimer Program