ROME – Efficient screening for potentially dangerous arrhythmias in adolescent and young-adult athletes requires the participant’s history, a physical examination, and results from a 12-lead ECG examination, based on experience with more than 15,000 screenings at one U.K. center.
"You need to use symptoms and the ECG results together," Jakir Ullah said at the annual meeting of the *European Association for Cardiovascular Prevention and Rehabilitation. "Either technique by itself is not best." Symptoms in sport participants who underwent screening were not associated with underlying cardiac pathology unless they occurred along with a group 2 ECG abnormality, said Mr. Ullah, a researcher at St. George’s University in London.
Most potentially dangerous cardiac abnormalities in adolescent or young-adult sport participants are asymptomatic, said Dr. Saqib Ghani, a cardiologist at St. George’s and a coinvestigator on the study. "ECG is more helpful than symptoms because you can miss the condition if it’s asymptomatic, and symptoms are very subjective," Dr. Ghani said in an interview.
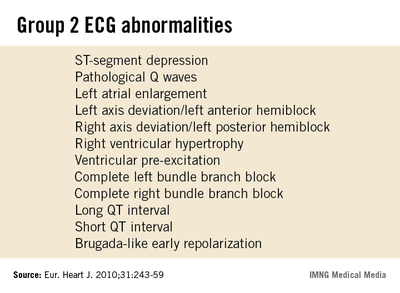
An expert panel organized by the European Association for Cardiovascular Prevention and Rehabilitation and the European Society of Cardiology compiled a list of 13 uncommon, potentially pathological ECG abnormalities, known as group 2 abnormalities, in 2010 (Eur. J. Cardiol. 2010;31:243-59). The list includes T-wave inversion, left atrial enlargement, a long QT interval, and right ventricular hypertrophy.
Together, these abnormalities occur in fewer than 5% of people screened by ECG prior to starting sport participation, according to data collected on more than 32,000 Italians aged 8-78 years who underwent pre–sport participation screening during 2003 (Eur. Heart J. 2007:28:2006-10).
Although many sports organizations call for preparticipation screening regardless of age or intensity level, cardiologists at St. George’s focused on people 14-35 years old because children under age 14 often show transient ECG abnormalities, while among adults over age 35 the main cardiac threat during sport participation comes from coronary artery disease rather than an abnormality, Dr. Ghani said.
 Mitchel L. Zoler/IMNG Medical Media
Mitchel L. Zoler/IMNG Medical Media
Mr. Jakir Ullah
The St. George’s series consisted of 15,027 people who were examined during 2007-2012. More than half of them were free of any ECG abnormality or symptoms and received immediate clearance for participation. But 6,598 people required further assessment, with 5,415 reporting symptoms, and 1,183 found with a group 2 ECG abnormality. The 8% prevalence rate for a group 2 abnormality, higher than in Italy, matches the somewhat higher U.K. prevalence rates reported by others, he added.
Among the 5,415 people investigated because of symptoms, none were found to have any underlying pathology that precluded sports participation, Mr. Ullah said. Symptoms included chest pain, syncope, palpitations, and dyspnea.
In contrast, among the 1,183 people identified for further assessment because of a group 2 ECG abnormality, the examination identified a clinically important underlying pathology in 67, 0.4% of everyone screened; another 44 people continue to undergo evaluations, and 1,072 people were found free of any sports-limiting condition. Among the 67 with an ECG abnormality and confirmed cardiac pathology, 25 (37%) also had symptoms. The most common cardiac pathology was Wolff-Parkinson-White syndrome, in 29 people, followed by a long QT interval in 8.
Dr. Ghani also stressed that ideally, pre–sport participation screening should occur for all sport participants regardless of the intensity of training or competition. "You only hear about sudden death in high-level athletes, but that is just the tip of the iceberg," he said. "We never know about the sudden death that happens to someone who is just running on the road."
Dr. Ghani and Mr. Ullah had no disclosures.
On Twitter @mitchelzoler
*Correction (5/29/13): A previous version of this story misstated the name of the meeting during which these presentations were given. This story has been updated.