News

CDC study finds 56% drop in HPV infections
Major finding: Among females aged 14-19 years, the prevalence of HPV infections dropped from 11.5% during the period prior to HPV vaccine...
For those senior pediatricians such as me, the importance of vaccines to
child and adolescent health such as Hemophilus influenzae, pneumococcal
vaccine and others is a "no brainer." We recall the devastating
diseases that are no longer commonplace, because of prevention by
immunization. In the United States, 14 million people will become
infected with HPV every year and 26,200 will develop new cancers from
HPV, almost half of these cervical cancer. As Dr. Frieden pointed out in
the telebriefing, even the small percentage of girls who have received
with the HPV vaccine has made a difference, reducing HPV infections by
almost 60% among females aged 14-19 years in just 4 years.
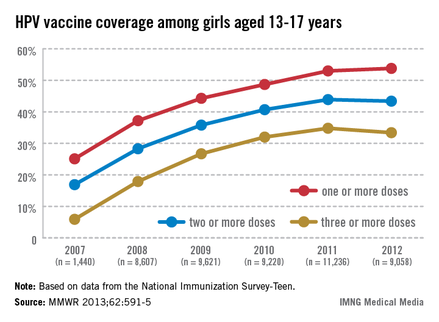
The HPV vaccine series has met with an initial difficult reception from parents, patients, and providers. Although, at first, the cost of approximately $380 for the three-shot series was a barrier, over time this has become less of an obstacle, and interestingly, this issue was not reported to be a barrier to receiving the vaccine series in the Centers for Disease Control and Prevention's Advisory Committee on Immunization Practices survey on the quadrivalent series. Current lassitude has resulted in only 33.4% of 13- to 17-year-olds being fully immunized in 2012, as reported in the MMWR.
In the same survey, missed opportunities to provide this vaccine after a girl's 11th birthday increased from 20.8% to 84%. Clearly, recommendations to refine systems of delivery in physicians' offices and the use of electronic health records (EHR) to prime providers to immunize at every opportunity in the clinical setting are good ideas. But an undercurrent that is often not openly discussed is that physicians often don't ask or wish to "take on" negative parental reaction to this important vaccine that can prevent cancer but is often linked to reproductive behavior. The link with acquisition of this virus through sexual activity is one that parents often don't want to consider, and frequently the provider acquiesces. In the ACIP survey, the most common reason cited by parents is that they do not believe the vaccine was necessary, followed by concerns of safety, that the vaccine was not recommended, lack of knowledge about the disease, and, finally, that their daughter was not sexually active.
Pediatricians must use every visit to review immunization status. When in an exam room, HPV should be included in the vaccines that are given at a health visit to prevent meningitis and pertussis. For example, say, "Maggie is due to receive these shots today; they are HPV, Menactra, and Tdap."* Too often, other physicians and I timidly approach the HPV vaccine series and allow parents' lack of knowledge - or worse, media hearsay - to dictate a youngster's care and, they opt to not immunize. Moreover, we often don't even have the conversation!
In the clinical trenches, if a parent questions why her daughter or son needs the vaccine, a directed but not overly lengthy response of the importance of this vaccine in preventing cervical and other cancers will inform the parent and teen, and is generally well received. Often, asking if an older family member or friend has suffered with cervical cancer will allow the parent to acknowledge that this is a reality that they do not want their teen to experience. When we fail to recommend the HPV series or say its fine "to wait" because of an inability and unwillingness to raise the link of acquisition of HPV and sexual activity, an opportunity is missed.
The media has done much to promote positive health behaviors, but sadly, parents often recall only the negatives associated with the HPV vaccine. Both clinicians and parents must repurpose themselves to protecting children and adolescents. Parents and youth rely on their pediatrician's recommendations and knowledge. In brief, pediatricians must pin a Post It note to their EHR to cue them to educate, but then vaccinate! In short, "Do Ask, Do Tell." No opportunity to protect our youth should be lost!
Dr. Susan Jay is program director of adolescent health and medicine at Children's Hospital of Wisconsin in Wauwatosa, and a professor of pediatrics at the Medical College of Wisconsin. Dr. Jay has no relevant financial disclosures.
*Correction 8/5/2013: The vaccine was misstated as DTap; teens receive Tdap.
This story was updated. 8/5/2013
FROM MORBIDITY AND MORTALITY WEEKLY REPORT
Major finding: Among females aged 14-19 years, the prevalence of HPV infections dropped from 11.5% during the period prior to HPV vaccine...