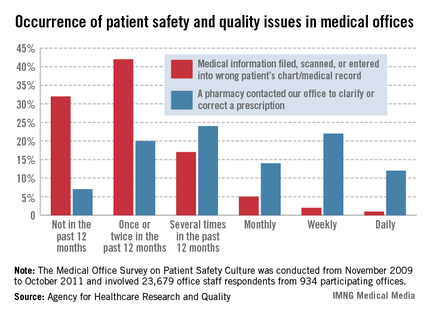
In a survey of office staff personnel, 8% said that medical information is filed, scanned, or entered into the wrong patient chart or record on at least a monthly basis, the Agency for Healthcare Research and Quality reported.
When 23,679 physicians and staffers were asked how often, in the past 12 months, data ended up in the wrong chart/record, 1% said it happened on a daily basis, 2% said it was a weekly occurrence, and 5% said it happened monthly. About 17% of respondents said that it had happened several times in the past 12 months, 42% said it had occurred once or twice in the past year, and 32% said that it had not happened at all, according to results from the Medical Office Survey on Patient Safety Culture.
Another question in the survey asked how often a pharmacy contacted the office to clarify or correct a prescription. This occurred daily for 12% of respondents, while 22% said it happened about once a week and 14% said it was a monthly occurrence. Another 24% of respondents said that there had been a pharmacy clarification/correction several times in the past year, 20% said it had happened once or twice, and 7% reported that there was no such contact, the AHRQ said.
The patient safety culture survey was conducted from November 2009 to October 2011. The respondents represented 934 medical offices, of which 62% had fully implemented an electronic medical/health records system and 73% were owned by a hospital or health system.