Preliminary draft of a new AF taxonomy
The consensus statement from the AFNET/EHRA group includes a draft of a new way to classify and think about AF. They divided AF into seven types: monogenic, focally induced, postoperative, valvular, AF in the elderly, polygenic, and unclassified (see table). But the coauthors of the statement cautioned that their proposed classifications were "preliminary," just a "step towards" a new AF taxonomy.
The proposed classification "is useful because it identifies patients with specific causes of AF, but it is preliminary because it is not able to classify many patients. We need better markers for the common mechanisms of AF," said Dr. Kirchhof in an interview. Progress in AF classification and taxonomy and progress in AF management will be "closely intertwined," he said. "We have a relatively decent understanding of several major mechanisms that cause AF, but we need clinically applicable markers that need to be validated. I expect that blood-based markers, and, to some extent, ECG-based markers will become helpful in the near future provided that they are validated."
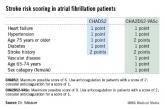
Factors already accepted as valid tools for discriminating among AF patients include myocardial ischemia, hemodynamic instability, blood cell count, electrolytes, thyroid stimulating hormone level, ECG, and the presence or absence of AF-related symptoms, while decisions about anticoagulation are driven by a patient’s CHA2DS2-VASc score.
According to the consensus statement, factors currently under development and seen as good candidates for additional ways to discriminate among AF patients include:
• More ECG-derived information including evidence of left ventricular hypertrophy, heart failure, QT interval, atrioventricular block, and cardiomyopathy, as well as analysis of the electrical complexity of AF episodes.
• Silent AF episodes detected by prolonged ECG monitoring with a miniaturized device; also using prolonged ECG monitoring to further refine and personalize rhythm-control therapy.
• Brain imaging, particularly magnetic resonance imaging (MRI), to identify silent brain infarctions, white matter hyperintensities, and cerebral microbleeds to further refine anticoagulant treatment.
• Structural heart disease including valve disease, left ventricular hypertrophy, and left ventricular dysfunction detected by MRI or three-dimensional echocardiography.
• Atrial activation time monitored by tissue Doppler to better guide rhythm-control treatment.
• Blood levels of D-dimer, high-sensitive troponin T, and forms of brain natriuretic peptide, biomarkers that might refine stroke-risk assessment and anticoagulation.
• Chronic kidney disease, which might especially affect stroke risk.
• Blood and urine biomarkers of inflammation, cardiac load, cardiac damage, or kidney function that may predict the risk of recurrent AF, including various forms of brain natriuretic peptide, C-reactive protein, and creatinine.
• Genes linked to familial forms of AF, such as genes close to the PITX2 locus on chromosome 4q25 and genes close to the ZFHX3 locus on chromosome 16q22.
What comes next?
Dr. Camm cited two methods in particular as among the closest to becoming the next new ways to assess and discriminate AF patients. One is evaluating atrial remodeling by MRI, which also identifies regions of atrial fibrosis. This is especially promising because several drug classes may stop or perhaps reverse fibrotic changes in atria: angiotensin-converting enzyme inhibitors, angiotensin-receptor blockers, and galectin 3 inhibitor drugs.
Another way to assess AF and personalize management nearing routine use is measuring ECG patterns on the atrial surface with noninvasive sensors placed on a patient’s chest, patterns that may pinpoint conduction lesions or circuits amenable to focused ablation.
It’s also very possible that some new, validated markers of AF will flag some of the earliest pathologic changes that start down the road to AF, markers that could identify potential targets for early intervention, "allowing us to interrupt the AF process before it becomes an end-stage disease and while it can still be more directly managed," Dr. Camm said.
The AFNET/EHRA group plans to reconvene early next year and every 2 years after that to update its assessment of AF personalization, he added.
"Even AF patients treated with the best available treatment today have unacceptably high mortality. Treatments targeting individual mechanisms that cause AF could improve this," Dr. Kirchhof said.
Dr. Kirchhof said he has received consulting fees and honoraria from more than a dozen drug and device companies. Dr. Camm said he has received consulting fees and honoraria from more than 20 drug and device companies. Dr. Gillis said she has received honoraria from Medtronic. Dr. Calkins and Dr. Kowey had no relevant disclosures.
mzoler@frontlinemedcom.com
On Twitter @mitchelzoler