From the Department of Neuropsychiatry and Behavioral Sceince, University of South Carolina School of Medicine, Columbia, SC.
Abstract
Objective: To review the identification, clinical assessment and treatment of patients with late-life depression.
Methods: Review of the literature.
Results: Depressive symptoms are present in up to 1 in 4 older adults. Comprehensive evaluation of depressive symptoms in this population often requires a multidisciplinary and collaborative approach between primary care, mental health, and other ancillary providers. Key aspects include a detailed history, physical and mental status examinations, cognitive and functional status assessment, and suicide risk assessment. Treatment options include anti-depressants, psychotherapy, and electroconvulsive therapy.
Conclusion: A systematic approach to evaluating depressive symptoms in the elderly can enhance timely recognition and treatment.
The U.S. population is aging, and with this comes the potential for increased health care needs. In 2014, there were over 46 million Americans age 65 and over (14.5% of the U.S. population). This number is projected to increase to 88 million by the year 2050 [1]. One in 4 older adults suffers with depressive symptoms that cause distress and functional impairment [2]. The World Health Organization Global Burden of Disease Study found depressive disorders to be the leading cause of disability-adjusted life years (DALYs) and the second leading cause of years lived with disability (YLDs). The burden of disease due to depressive disorders increased by 37.5% between 1990 and 2010, and 10.4% was attributable to aging [3]. These figures underscore the importance of accurate assessment and treatment of depression in the elderly. In this article, we review the identification, clinical assessment, and treatment of patients with late-life depression.
Diagnostic Criteria
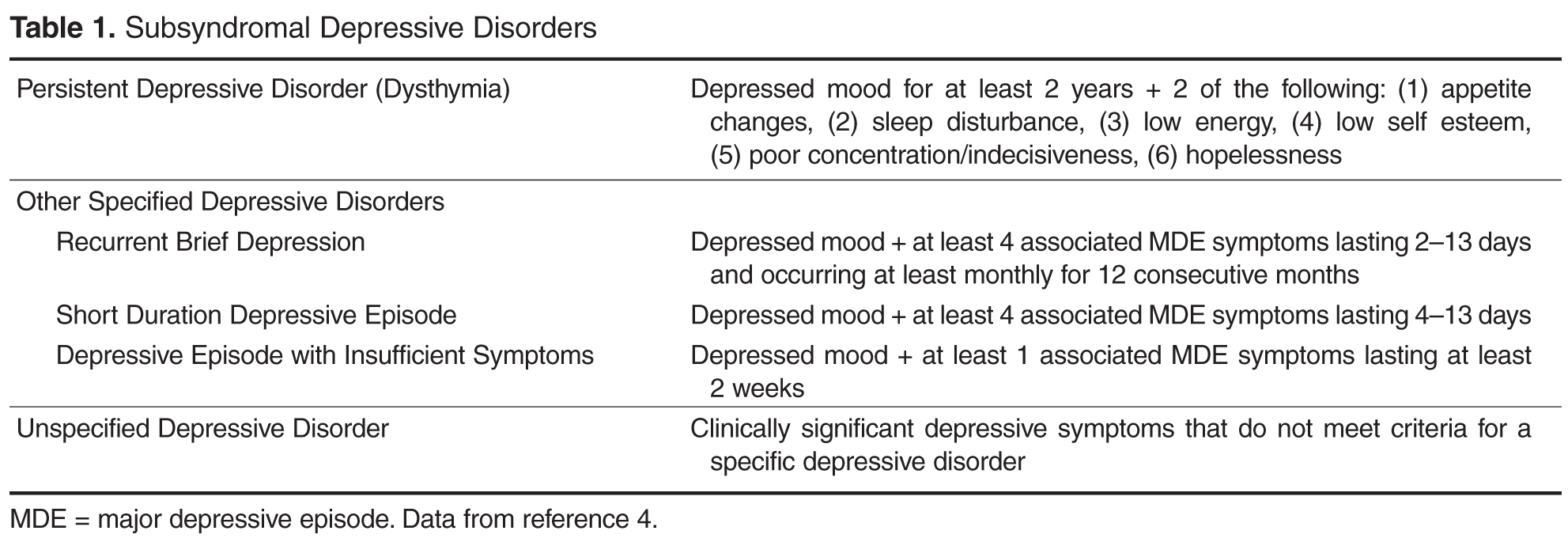
Late-life depression (LLD) is defined as onset of depressive symptoms after age 65 years. The Diagnostic and Statistical Manual of Mental Disorders, 5th edition (DSM-5) criteria for major depressive disorder (MDD) is unchanged from the DSM-IV, text revision (DSM-IV-TR) criteria. In order to receive a diagnosis of major depressive disorder, patients must exhibit depressed mood and/or loss of interest plus 4 or more associated symptoms, including changes in appetite, sleep disturbance, psychomotor agitation or retardation, fatigue, inappropriate guilt or feelings of worthlessness, poor concentration or indecisiveness, and recurrent thoughts of death or suicidal ideation. Symptoms must be present nearly every day for at least 2 weeks and cause clinically significant distress or functional impairment [4]. Patients who do not fully meet criteria but still exhibit clinically significant distress may be diagnosed with various subsyndromal depressive disorders ( Table 1 ).
Prevalence
It is estimated that 1% to 4% of community-dwelling adults age 65 and older suffer from MDD, with women more likely to be affected than men (prevalence of 4.4% vs. 2.7) [2,5–7]. This estimate is low compared with lifetime prevalence of almost 20% in the general adult population [8]. However, when depressive symptoms that do not meet criteria for MDD are considered, prevalence rates increase up to 25% [2,9]. These estimates also vary by clinical setting, with the highest rates (up to 40%) among elderly patients in long-term care facilities [10,11]. While individuals with subsyndromal depression may experience fewer symptoms than those with MDD, clinically significant distress persists, impacting health and functional status. Depression is associated with overall poor social or occupational functioning, cognitive decline, increased health care utilization and cost, increased morbidity and mortality from medical illness, and increased suicide mortality [5,9,10,12].