Cardiovascular Risk Reduction in Patients with Type 2 Diabetes
Journal of Clinical Outcomes Management. 2017 February;24(2)
References
What secondary prevention of cardiovascular disease is recommended for patients with T2DM?
Optimal secondary prevention following a major vascular event includes a combination of pharmacologic and nonpharmacologic interventions. In the population without diabetes, evidence supports smoking cessation, exercise, cardiac-specific rehabilitation, antiplatelets, RAAS antag-onists, beta-blockade, and statins. Most of the trials that led to this standard suite of interventions had large diabetes subgroups. Therefore, there is no difference in the secondary prevention of cardiovascular disease in the population with diabetes with regard to these interventions.
Have any antihyperglycemic agents been shown to reduce cardiovascular events?
Metformin
Due to its long history and safety profile, metformin is considered the first-line antihyperglycemic agent in most of the developed world. Despite this, there are few high-quality studies specifically assessing the efficacy of metformin at decreasing cardiovascular event rate. The landmark UKPDS trial compared intensive to conventional glycemic therapy. In a substudy, 753 overweight patients were randomized to metformin or conventional therapy. Diabetes-related death, all-cause mortality, and any diabetes endpoint were all decreased significantly in the metformin group [13]. Furthermore, 10 years of post-trial observational follow-up showed continued benefit in the metformin group despite loss of difference in glycemic control [14]. However, the cardiovascular benefit of metformin in the current era is controversial, with conflicting results from different meta-analyses [61,62].
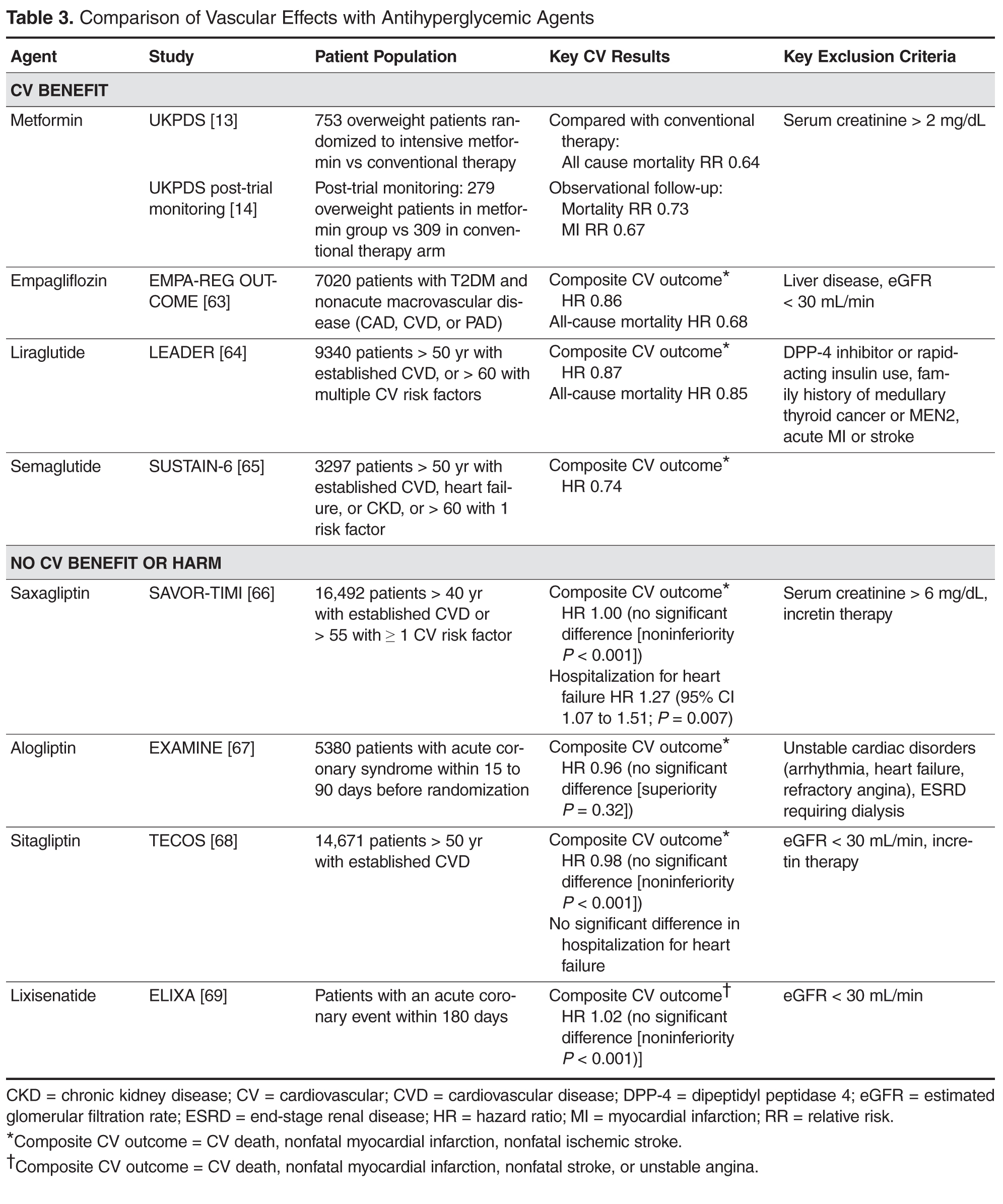
A summary of the vascular effects observed during trials of antihyperglycemic agents is shown in Table 3 .
Empagliflozin
Many large randomized, controlled cardiovascular outcome trials have been completed or are ongoing looking at the cardiovascular safety of newer antihyperglycemic agents. The majority of the completed trials have shown a neutral effect, suggesting that the agents are safe. However, in September 2015, the first cardiovascular outcome trial of an antihyperglycemic agent with a positive result was published. The Empagliflozin Cardiovascular Outcome Event Trial (EMPA-REG OUTCOME) randomized 7020 patients with T2DM and cardiovascular disease (defined as nonacute myocardial infarction, multivessel coronary artery disease, unstable angina, nonacute stroke, or occlusive peripheral arterial disease) to placebo or 1 of 2 doses of empagliflozin. The primary outcome of cardiovascular mortality, nonfatal myocardial infarction, or stroke was reduced by 14% in the empagliflozin-treated group. Key secondary outcomes of all-cause mortality (HR 0.68) and heart failure hospitalization (HR 0.65) were also statistically different in favor of the empagliflozin arm [63].
On the basis of this trial’s results, empagliflozin should be considered for treatment of all patients with type 2 diabetes and known cardiovascular disease. It is as yet unknown whether this effect will translate to the other members of the sodium-glucose co-transporter 2 (SGLT-2) inhibitor class, although results of studies involving other SGLT-2 inhibitors are expected in the next 2 to 3 years.
Liraglutide
In 2016, the Liraglutide Effect and Action in Diabetes: Evaluation of Cardiovascular Outcome Results (LEADER) trial reported results of its cardiovascular safety trial. In this trial, 9340 patients with either established vascular disease or risk factors for vascular disease were randomized to daily liraglutide or placebo injections. The primary composite outcome of cardiovascular death, nonfatal myocardial infarction, or stroke was reduced by 13%. A key secondary outcome of all-cause mortality also showed a significant reduction (HR 0.85). There was no reduction in hospitalization for heart failure [64].