Journal of Clinical Outcomes Management. 2016 May;23(5)
References
Although having acne during puberty is not considered as a marker for hyperandrogenemia, patients with moderate to severe inflammatory acne that is poorly responsive to topical treatment should be evaluated for underlying hyperandrogenemia [19,24,25].
What laboratory tests should be obtained to when there is clinical suspicion of hyperandrogenemia?
As with the variability in clinical symptoms, there is a lack of uniformity regarding biochemical testing for this disorder. There is no consensus on which biochemical tests should be done in girls suspected of having PCOS. For the initial evaluation of hyperandrogenemia, measurement of total and/or free testosterone is recommended [13,26–28]. Elevated free testosterone is recognized as the single most sensitive indicator for hyperandrogenemia, as the free fraction is the bioactive portion of serum testosterone. Most circulating testosterone is bound to sex hormone–binding globulin (SHBG), and obesity and androgen excess lower the level of SHBG, thus increasing free testosterone fraction. Clinical evidence of virilization should prompt a workup for disorders mimicking PCOS ( Table 2 ) [27]. Obtain baseline thyroid and prolactin levels in any adolescent with chronic anovulation to exclude hyperprolactinemia and thyroid disorders. Most patients with PCOS have higher luteinizing hormone/follicle-stimulating hormone (LH/FSH) ratio; however, the test does not have robust diagnostic utility due to the variability of serum LH levels commonly seen during the different stages of the menstrual cycle. In addition, no difference in LH/FSH ratio was found in a group of obese PCOS patients when compared with a control group [29]. Given the increased association of obesity with PCOS, evaluation for metabolic syndrome is crucial. Laboratory testing requires reliable assays with well-defined normal ranges, especially for free testosterone since the assays are less well standardized, which limits their usefulness [13]. Table 2 provides a comprehensive list of recommended testing that should be tailored to the patient’s presentation.
Case Continued
The patient underwent laboratory assessment that included total and free testosterone levels, lipid panel, thyroid studies, prolactin level, comprehensive metabolic panel (CMP) and hemoglobin A1c (HbA1c). Due to lack of virilization, she was not tested for PCOS-like syndromes. Her total and free testosterone were 90 ng/dL (normal, < 41) and 24.7 pg/mL (normal, 0.5–3.9) respectively. Thyroid-stimulating hormone and prolactin levels were normal. She had normal lipid levels and CMP but HbA1c was 5.9% (pre-diabetic range). The results of a 2-hour oral glucose tolerance test revealed a level of 160 mg/dL, indicative of impaired glucose tolerance.
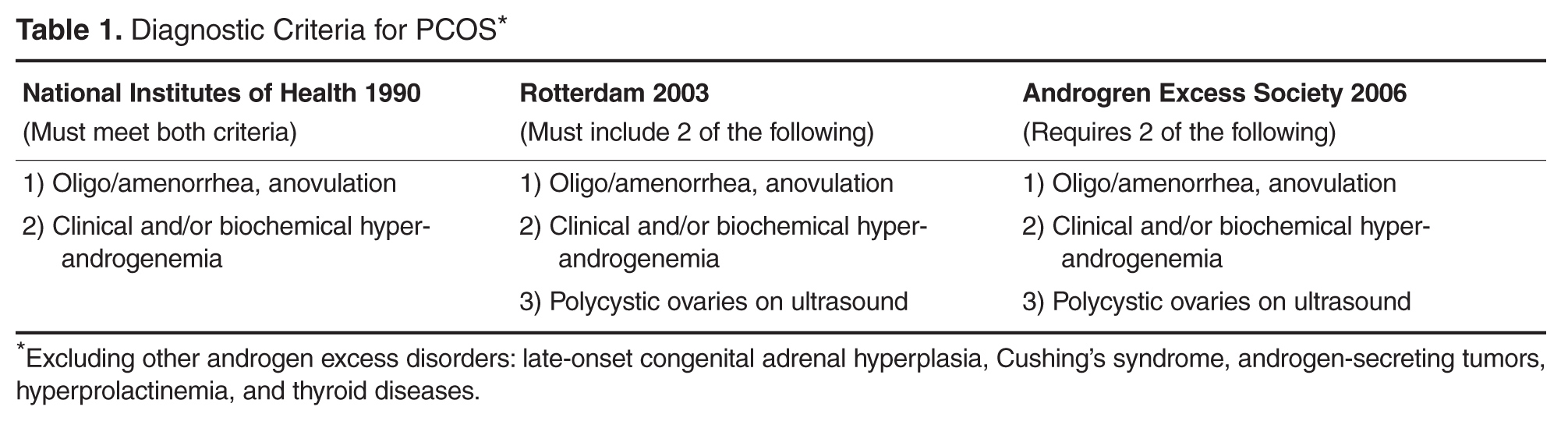
What is the pathophysiology and diagnostic criteria for PCOS in adolescents?
PCOS has diverse etiology and has been linked to both genetic and environmental factors affecting ovarian steroidogenesis [13,30]. While the familial clustering strongly supports the role of genetic factors, variability in phenotypic features within the same or different families indicates the importance of environmental contribution [31–34].
The exact underlying mechanism leading to disruption of ovulation is still unclear; however, hyperinsulinemia augmenting ovarian androgen production has been well recognized [35–37]. Insulin resistance is a characteristic finding in PCOS and occurs both in obese and lean patients [38,39]. Obesity further exacerbates the insulin resistance state in PCOS patients. Therefore, obese patients with PCOS have more severe hyperandrogenemia and consequences from it (hirsutism, menstrual abnormalities, and metabolic derangements) than normal-weight PCOS patients [40,41]. Similar to LH, insulin can stimulate ovarian theca cells directly and cause increased production of androgens [42]. Elevated androgen levels cause the irregular menstrual periods as well as clinical signs of hyperandrogenemia, such as hirsutism and acne.