Clinician Telephone Training to Reduce Family Tobacco Use: Analysis of Transcribed Recordings
Journal of Clinical Outcomes Management. 2016 February;23(2)
References
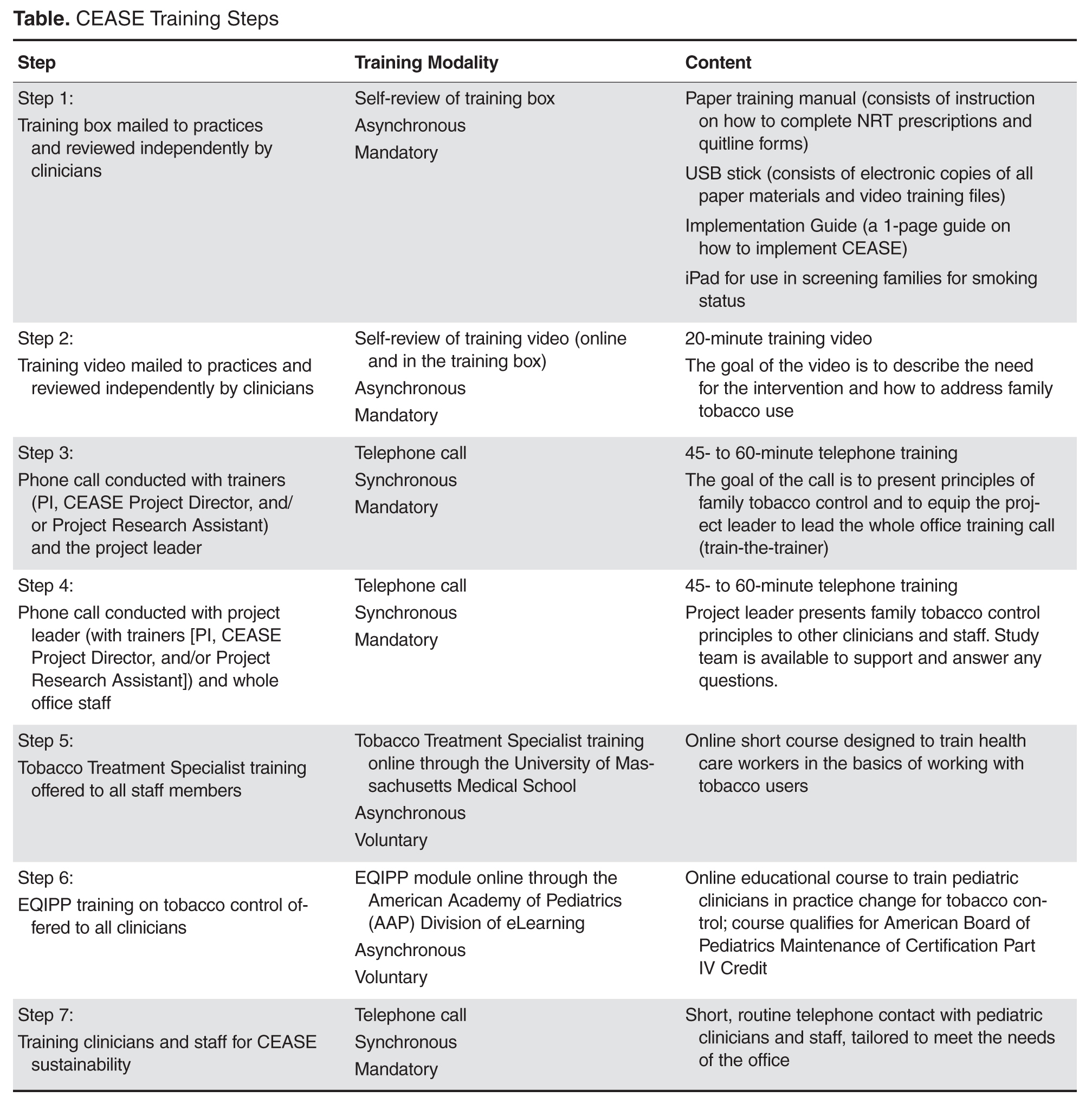
The CEASE intervention works with pediatric primary care offices on strategies to promote routine and effective family-centered tobacco control by addressing parental smoking and establishing smoke-free home and car rules. Based on national guidelines and extensive data obtained in previous pilot testing [12,14–16], elements of the CEASE intervention have been designed to be adapted to individual practices’ staffing, resources, and physical configuration. The main elements of the intervention are identifying tobacco users and children exposed to tobacco smoke through the use of a paper or an electronic tablet screening tool, assisting smokers in setting a quit date, establishing rules for smoke-free homes and cars, prescribing nicotine replacement therapy (NRT) to help smokers cut down or quit [17,18], referring smokers to tobacco quitlines and/or the SmokeFreeTXT program [19–25], and following up with tobacco users. Clinicians and staff are trained in the adoption, implementation, and maintenance of family-centered tobacco control strategies with the goal of embedding the elements of CEASE intervention into routine practice beyond the training and/or research study periods. The CEASE training was designed to meet the needs of pediatric offices, be time- and cost-effective, and be implemented through distance learning strategies to save both trainer and pediatric office staff resources. The training approach consists of a number of evidence-based strategies. As depicted in the Table, the training involves multiple modalities, including videos, reference materials, online computer education modules, and telephone training calls.
One of the more innovative aspects of CEASE has been the use of training calls. In studies of CEASE, the peer-to-peer call was conducted by the principal investigator with the project leader at the practice using a train-the-trainer model. After the project leader was trained through the peer-to-peer call, the project leader then led the whole office training call, with the support of CEASE staff by phone. The training calls worked in conjunction with the other aspects of the training, as shown in the Table. The training calls for the practices provided a valuable research opportunity. We examined the concerns and issues that clinicians and office staff had about implementing an office-wide tobacco control program through a qualitative analysis of the call transcripts. This paper outlines the main considerations and questions that clinicians and office staff expressed during the training calls. Understanding the points of view of clinicians and staff will help researchers and clinical educators strengthen the design of tobacco control interventions.
Methods
Study Aims
The data for this paper were collected as part of a larger mixed-methods controlled trial. The overarching aims of the trial were to study implementation and sustainability of tobacco-control services delivered at the clinic level, to facilitate behavior change among parents and evaluate cost-per-quit among parents who smoke, and to study systems changes and the processes that affect them at the practice level. The study was conducted in 5 intervention and 5 control pediatric primary care practices in 5 states; this paper reports on data collected in intervention practices and focuses on understanding the systems changes and processes that are instituted when implementing a tobacco control program at the clinician and practice level.