Management of Acute Decompensated Heart Failure in Hospitalized Patients
Journal of Clinical Outcomes Management. 2015 April;22(4)
References
) [12–16]. These predictor models emphasize the importance of early identification of high-risk patients, which may allow for focusing intensity of care where it is most needed. Prospective studies will be needed to determine to what degree risk stratification may improve outcomes.
Case Continued
Upon further evaluation by a cardiologist, the patient is cool and clammy with elevated neck veins and prominent S3 confirmed. She continues to report severe shortness of breath after 1 dose of intravenous (IV) furosemide in the ED. Repeat vital signs shows a blood pressure of 83/49 mm Hg and respiratory rate of 33. Her electrocardiogram shows sinus tachycardia. The cardiologist determines that the patient’s clinical profile is “cold and wet” and admits the patient to the cardiac care unit (CCU) with a diagnosis of ADHF.
Initial blood tests show a BNP level of 1830 pg/ml, troponin I is 0.63 and stable after 2 measurements, serum creatinine is 1.6 mg/dL, BUN is 44 mg/dL, and serum sodium is 132 mg/dL. The GWTG-HF risk score for in-hospital mortality was calculated based on admission data and the probability of death was estimated at > 5% to 10% [12]. Prompt aggressive medical therapy was instituted in the CCU consisting of furosemide infusion to reduce congestion and IV dobutamine to improve systemic perfusion. Enoxoparin 40 mg subcutaneously once daily was initiated for venous thromboembolism prophylaxis.
What are important aspects of therapy for ADHF?
Several days to weeks prior to the appearance of signs and symptoms of volume overload, patients may develop hemodynamic congestion, defined as an elevation of ventricular filling pressure/pulmonary capillary wedge pressure independent of clinical evidence of fluid overload [17]. Elevated filling pressure is the culprit in the development of most of the signs and symptoms of ADHF and is the target for treatment.
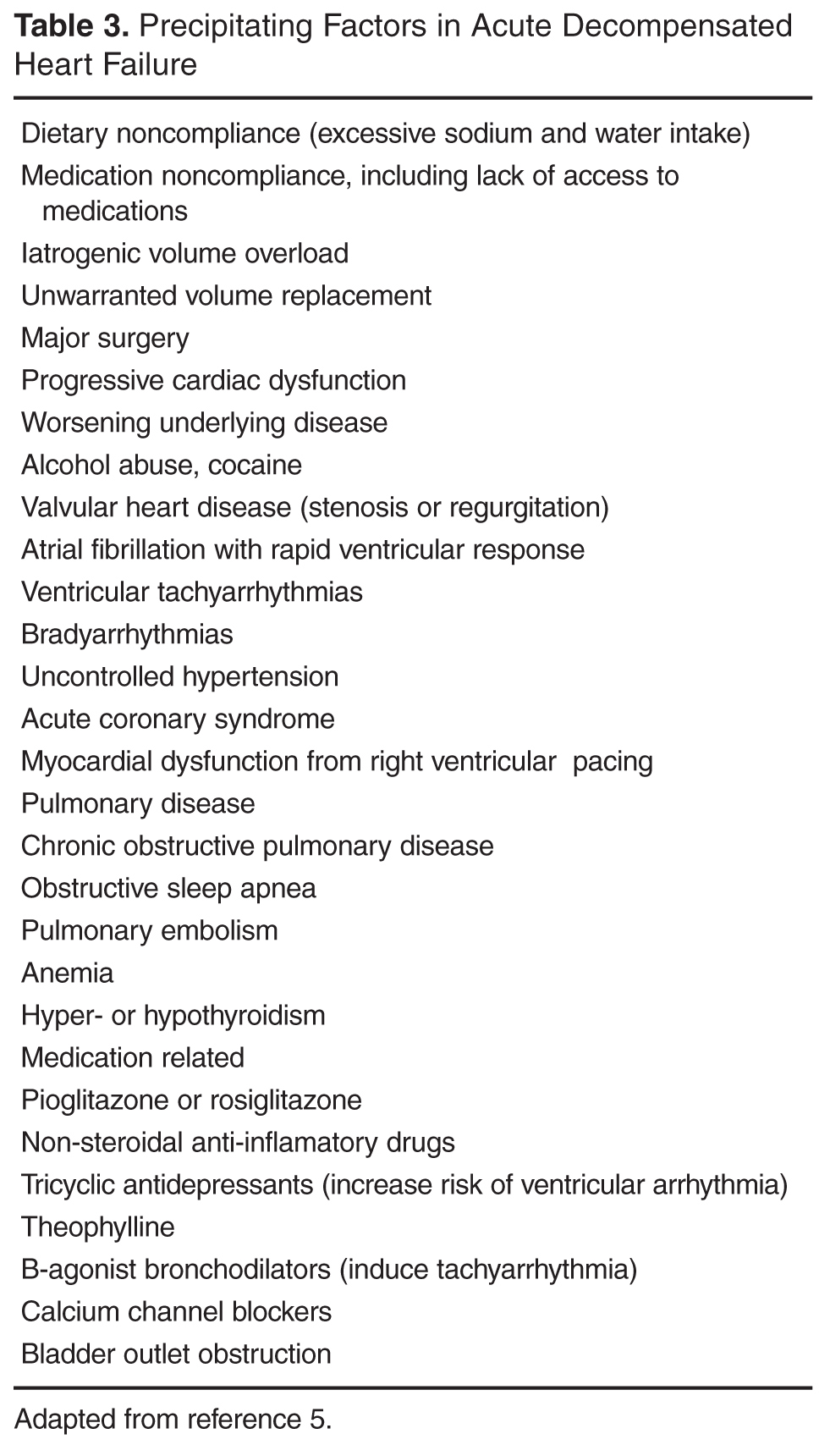
An important aspect in the management of ADHF is identifying precipitating factors and/or comorbid conditions ( Table 3 ) and treating them appropriately in conjunction with volume overload [5]. Echocardiogram is a widespread and readily available diagnostic tool providing important information on systolic and diastolic ventricular function as well as other structural heart disease abnormalities. Additionally, myocardial ischemia evaluation with noninvasive testing or cardiac catheterization should be performed if ischemia is a potential contributor to the patient’s heart failure symptoms. The most common cause of heart failure readmission is noncompliance with medications or dietary restrictions. Hospitalization provides an opportunity to educate the patient about their condition and rationale for therapy as well as identify barriers to appropriate self-management.
Although use of vasoactive medications such as nitroglycerin or nitroprusside are not routinely recommended for use in all ADHF patients admitted to the hospital, retrospective analysis of the ADHEREdatabase suggests that there is a significant reduction of mortality, hospital length of stay, admission to intensive care unit, invasive procedures, and prolonged hospitalizations when IV diuretics, vasodilators (nitroglycerin, nitroprusside, nesiritide,) and/or positive inotropes (milrinone, dobutamine) are initiated in the ED within 6 hours of an ADHF presentation [18,19].However, whether prompt ED intervention impacts intermediate- to long-term outcomes is unknown [4].