Journal of Clinical Outcomes Management. 2014 October;22(10)
References
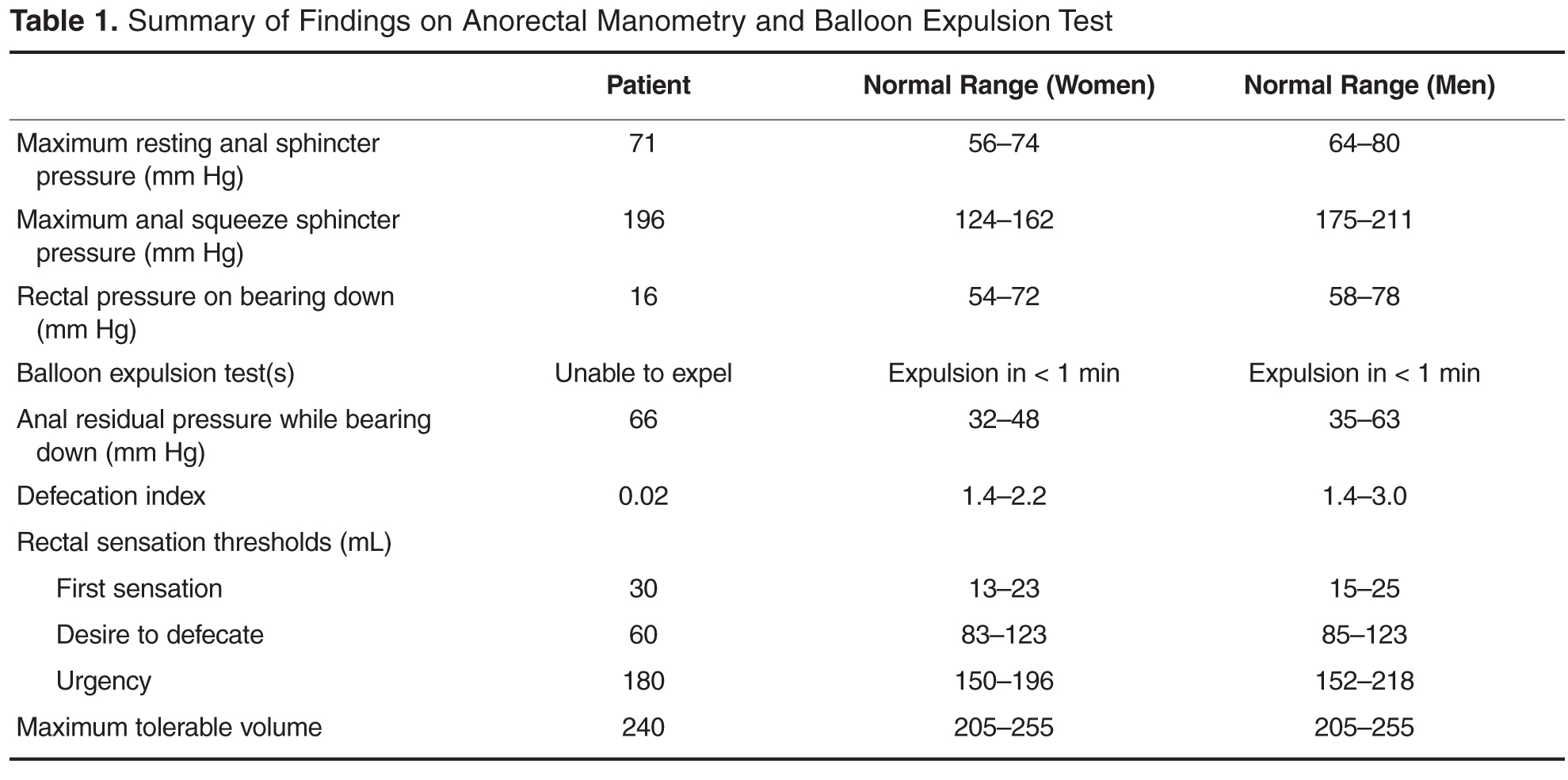
Normal subjects can expel a 50-mL water-filled balloon in less than 1 minute. Although normal patients can show a dyssynergic pattern in the left lateral decubitus position, when seated on a commode and with a sensation of stooling most exhibit a normal pattern of defecation [9].
Diagnosis
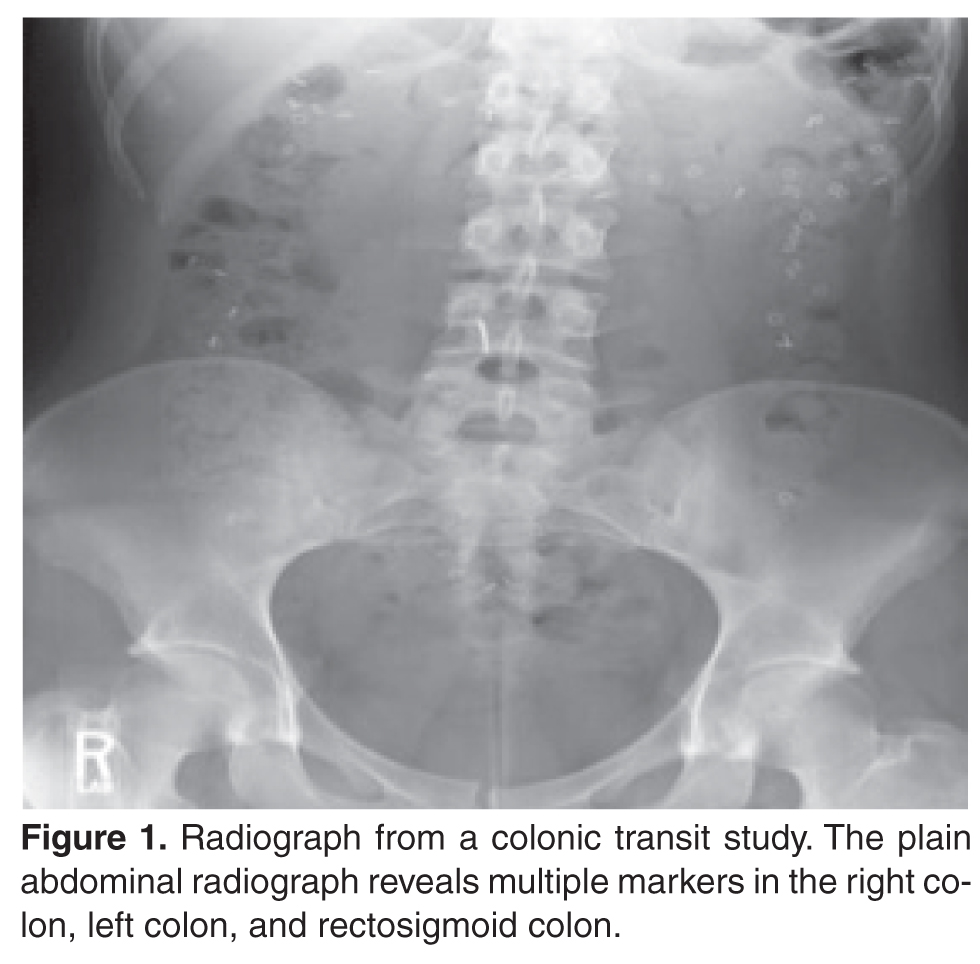
The case patient undergoes a colonic transit study and has several retained markers distributed primarily in the left colon ( Figure 1 ). Defecography shows incomplete relaxation of the puborectalis, with only 10% of the rectal contents expelled during the study. The results of anorectal manometry and the balloon expulsion test reveal normal sphincter pressures but evidence for an abnormal defecation pattern or dyssynergia: low defecation index (calculated by dividing the rectal pressure by the anal residual pressure during straining) and prolonged balloon expulsion time ( Table 1 ). Based on these findings, a diagnosis of dyssynergic defecation is made.
What treatment options are available for dyssynergia?
The treatment of patients with dyssynergic defecation consists of standard therapies for constipation, including diet, laxatives, and timed toileting. Medical therapy includes laxatives, polyethylene glycol, and lubiprostone.
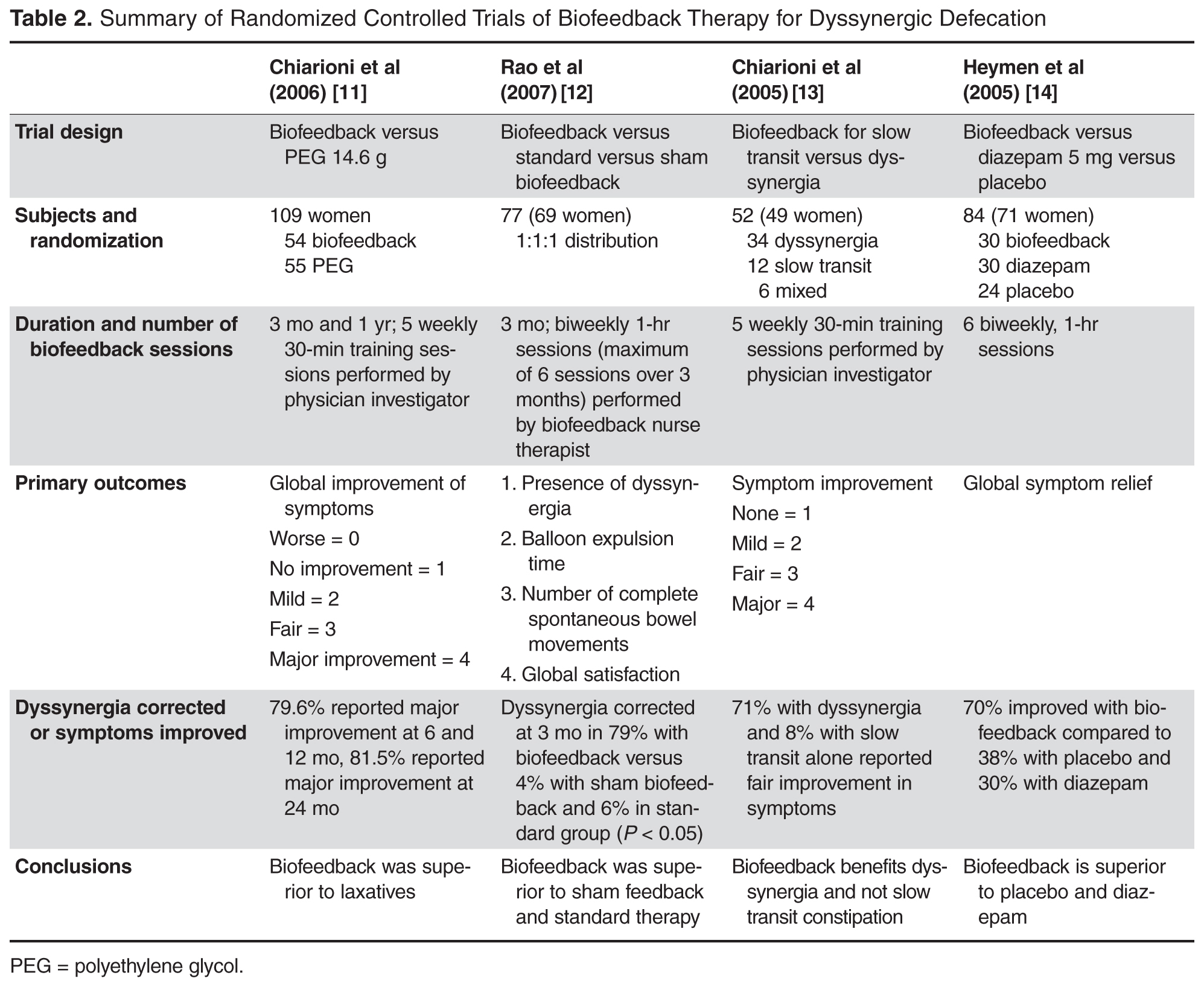
Biofeedback therapy is useful and efficacious. Its purpose is to restore a normal pattern of defecation by using an instrument-based education program. The primary goals are to correct dyssynergia and improve rectal sensory perception. Diaphragmatic muscle training, simulated defecation, and manometry- or electromyography-guided anal sphincter and pelvic floor relaxation techniques will improve symptoms in more than 70% of patients [11–13]. Table 2 summarizes data from recent published trials on the efficacy of biofeedback [11–14]. Other avenues of treatment include botulinum toxin injection and surgical approaches that are generally ineffective [15,16].
Case Study 2
Initial Presentation and History
A 39-year-old woman presents with a 5-year history of intermittent bright red blood with stooling. Most often, she notices blood on the toilet paper or when wiping and rarely in the commode. She reports having experienced difficulty with bowel movements since her teens. She does not have a daily urge but strains up to 30 minutes to pass stool that is hard in consistency (type 1–2 on the Bristol stool scale). Over the past year, she has started using fingers to remove stool.
The patient reports bloating and abdominal discomfort that is improved with stooling. Her weight has been stable. Current medications include polyethylene glycol 17 g twice daily, sodium docusate 100 mg twice daily, iron sulfate 325 mg 3 times daily, and a birth control pill. Her past medical history is significant for iron deficiency anemia. Family history is notable for her mother and sister with similar “bowel troubles,” but no family history of inflammatory bowel disease or colorectal cancer. She is a salesperson and has been married for 7 years. She does not use tobacco or alcohol. As a child, she was sexually abused. She did not receive any formal counseling for the abuse. Review of systems is negative.
Physical Examination
General and neurologic examinations are normal. The abdomen is mildly distended, bowel sounds are normal, there is mild tenderness, and stool is palpable in the left lower quadrant. Rectal examination reveals normal anal skin with no fissures, intact anocutaneous reflex, and hard stool in the rectal vault that is guaiac-positive. The resting anal sphincter tone is elevated, and when asked to attempt defecation, there is excessive perineal descent and rectal mucosal intussusception with paradoxical anal contraction.