FIGURE 1 Pre—uterine-artery-embolization arteriograms
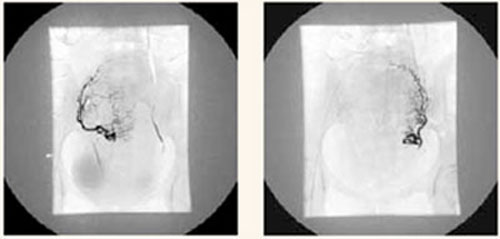
Preprocedure right and left arteriograms for vasculature of a 12-week size fibroid uterus.
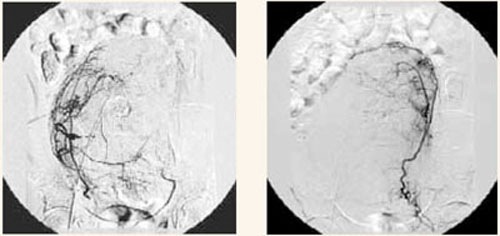
Preprocedure right and left arteriograms for vasculature of a 24-week size fibroid uterus.
FIGURE 2 Embolization catheter infusing microparticles within uterine artery
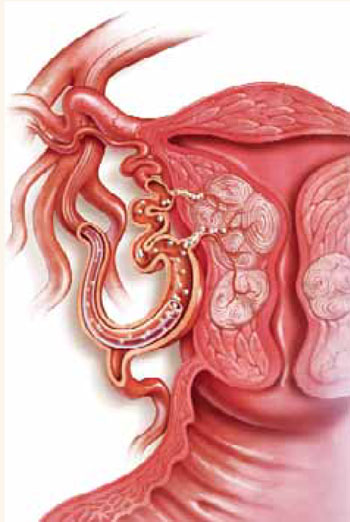
A catheter is passed into the right femoral artery, through the right external iliac artery to the aorta, then down the left common iliac artery to the left internal iliac, down the anterior division to the left uterine artery. Embolization material—polyvinyl alcohol particles or acrylic copolymer beads—is then delivered via catheter in the uterine artery until slow flow or stasis occurs in the artery.
Indications
Like hysterectomy and myomectomy, the indications for UAE are symptomatic fibroids that are unresponsive to medical management (with hormonal agents or analgesics). Common symptoms of fibroids include abdominal or pelvic pain, abnormal menstrual bleeding, anemia, urinary frequency, dyspareunia, and infertility.
UAE may be an especially useful option for women who are poor surgical candidates or have extensive adhesive disease, as well as for those who refuse blood products or are perimenopausal.6,8,9
Contraindications
Pelvic infection, severe contrast allergy, arteriovenous shunting, the presence of an undiagnosed pelvic mass, coagulopathy, renal insufficiency, a history of pelvic radiation, and genital tract malignancy all are contraindications.
Because data are limited on the safety of pregnancy following UAE, some authorities consider the desire for future fertility a relative contraindication.4,7,10
Preoperative evaluation
The preoperative workup should include a thorough history and physical examination by both an interventional radiologist and a gynecologist, a pregnancy test, pelvic imaging via ultrasound or magnetic resonance imaging, and endometrial biopsy to exclude endometrial hyperplasia or cancer. (Patients without abnormal bleeding may not require an endometrial biopsy.)
Outcomes
The average reported symptom improvement is 87%, and the mean reduction in fibroid volume is 46%.1 Most patients see improvement within 3 months of the procedure, with control over the symptoms lasting at least 2 years. At 1 year, 90% of patients report improvement in heavy menstrual bleeding.4
Most patients are discharged within 24 hours of the procedure, compared with 48 to 72 hours for abdominal hysterectomy or myomectomy. They also experience an average recovery period of 8 days, compared with 4 to 6 weeks for abdominal hysterectomy or myomectomy.6
However, a recent study found that women undergoing embolization for fibroids were more likely than those undergoing myomectomy to need further invasive treatment (i.e., repeat embolization or surgery) within 3 to 5 years (29% versus 3%).11
Complications
Most patients report some degree of “post-embolization syndrome,” which is characterized by low-grade fever, pain, malaise, nausea, and leukocytosis, generally within the first 4 days.4 This may be caused by the systemic effects of transient fibroid and uterine ischemia. Although the condition is usually self-limiting and observable on an outpatient basis, these patients are often admitted for antibiotic therapy.
“Post-embolization syndrome” is characterized by low-grade fever, pain, malaise, nausea, and leukocytosis, generally within the first 4 days.
In the most recent series published,12 major complications occurred in 0.5% of embolizations performed for symptomatic fibroids. They include pulmonary embolism, arterial thrombosis, groin hematomas, local infection, guide-wire perforation of arteries, allergic reaction to contrast medium, endometritis, ischemia of pelvic organs, sepsis, and death. Among more than 30,000 procedures performed to date worldwide, there have been 4 related fatalities. In 2 cases, pulmonary embolism occurred within a few days of the procedure; the 2 other deaths occurred within 2 weeks and were related to septicemia and disseminated intravascular coagulation.
There have been reports of total uterine necrosis, transient and permanent ovarian failure, and external sexual dysfunction. These complications may occur up to 2 years after the procedure.1,4,7,10,13-16 Nontarget vascular embolizations of the gluteus muscle, ovaries, labia minora, and bladder wall also have been noted.17,18
When viewed in the context of the large number of procedures performed—and considering the complications associated with myomectomy and hysterectomy—these rare complications show that, overall, UAE is a very safe procedure.
Pregnancy after embolization
Because we lack controlled studies and abundant data, the role of UAE in women contemplating childbearing is unclear. More studies are needed before UAE can be confidently recommended for these women. Premature ovarian failure is an uncommon but recognized complication of UAE.13
Several series and case reports have noted successful pregnancies following UAE.19,20 Our recent report21 on 50 pregnancies following UAE for leiomyomata noted higher rates of cesarean delivery, preterm delivery, malpresentation, spontaneous abortion, and postpartum hemorrhage than in the general population (TABLE). It is unclear whether the increased rate of premature delivery and malpresentation is due to residual fibroids, changes in myometrial vascularity or elasticity, or other unknown labor-associated processes.