FIGURE 1Sample voiding diary of a patient with complaints of urinary frequency, nocturia, and rare stress incontinence
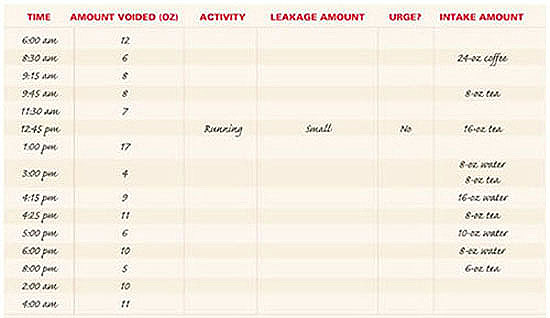
This sample diary alone reveals that symptoms were due to excessive fluid and methylxanthine intake. This patient’s symptoms abated with decreased intake of water and tea.
Physical examination
Perform a complete physical exam, focusing attention on elements specific to pelvic floor disorders.
Definitions of continence terms4
The International Continence Society periodically reports on terminology for the symptoms, signs, and urodynamic observations of pelvic floor disorders.1
| Urinary incontinence | Any involuntary leakage of urine |
| Stress urinary incontinence | Involuntary leakage of urine on effort or exertion |
| Urge urinary incontinence | Involuntary leakage accompanied by or immediately preceded by urgency |
| Urgency | A sudden compelling desire to pass urine that is difficult to defer |
| Mixed urinary incontinence | Involuntary leakage associated with urgency and also with exertion, sneezing, or coughing |
| Anal incontinence | The inability to control passage of flatus or liquid or solid stool |
Stress test. If the patient relates a history of stress incontinence, the condition must be documented before any anti-incontinence procedure is considered. One simple method for this is a stress test.
Ask the patient to present for her office visit with a full bladder, as if she had an ultrasound appointment. At the start of the physical exam, perform the stress test with the patient in a standing position. (The full bladder should reduce false-negative results.)
Have the patient stand with 1 foot on the step of the examination table. Now, sit on a stool and separate the labia with 1 hand, so that the urethral meatus is visible. (A 4×4 gauze in the other hand can absorb any urine that is lost.) Have the patient cough forcefully several times while you observe the meatus for loss of urine. A spurt of urine coincident with the cough is a positive test.
If the patient has a significant amount of prolapse—i.e., stage III or IV)—repeat the stress test with the prolapse reduced to eliminate the effect of any urethral kinking. (The prolapse can be reduced using the posterior blade of a speculum.)
After the stress test, have the patient void in a measured device, such as a toilet hat, to record the voided volume. When she returns to the examination room, obtain a postvoid residual (PVR). The stress-test volume is determined by adding the volume voided to the PVR volume.
Postvoid residual volume. This assessment enables the clinician to determine the bladder’s ability to empty. Physicians can measure residual urine either by catheterization or ultrasound. When using ultrasound, perform transabdominal imaging in the transverse and mid-sagittal planes. Once you have obtained measurements of the bladder’s diameter in 3 planes (anterior-posterior, transverse, and sagittal/longitudinal), you can approximate the volume using this formula:
Volume (mL) = height (cm) × length (cm) × width (cm) × 0.52
If no bladder dimension is greater than 5 cm, the PVR is less than 65 mL.
In our opinion, documentation of the PVR is a prerequisite for any incontinence or anterior/apical prolapse procedure; the clinician will need this information to interpret any postoperative voiding difficulties and to counsel patients at increased risk of such difficulties.
Neurologic examination. Although it is unlikely that significant neurologic disease contributes to the patient’s pelvic floor dysfunction, the ramifications of any disease can be substantial. Thus, perform a focused neurologic exam to evaluate mental status, lower-extremity and perineal sensation, and reflexes. The 2 relevant spinalcord reflexes are the bulbocavernosus and the anal wink.5 Interpret these tests with caution, however, since an anal wink may be absent in some women who are otherwise neurologically normal.6
Simple office tests
POPQ exam. In addition to the standard gynecologic examination, patients complaining of or presenting with prolapse should undergo an objective measurement of the problem: the pelvic organ prolapse quantitative (POPQ) exam.
In 1996, the ICS published standardized terminology that has been adopted by most specialty organizations.7 This POPQ system describes the location and severity of prolapse using segments of the vaginal wall and external genitalia, rather than the terms cystocele, rectocele, and enterocele (FIGURE 2).
While the patient is straining, 6 specific sites are evaluated. Measure each site (in centimeters) in relation to the hymenal ring, which is a fixed, easily identified anatomic landmark. The hymenal ring is the zero point of reference. If a site is above the hymen, it is assigned a negative number; if it prolapses below the hymen, the measurement is positive.
In women with stress urinary incontinence, it is important to determine whether urethral hypermobility is present.
Use a Sims speculum or the posterior blade of a bivalve speculum to isolate the different vaginal compartments. An inexpensive disposable wooden spatula (Pap smear stick) marked with centimeters works well as the measuring device.